Synthetic Duo: Synthetic enzymes and synthetic morphogenesis
A deformity of the hip joint caused by Legg-Calvé-Perthes' disease (LCPD) may cause reduction of the function of the joint, pain and future arthrosis which will necessitate a prosthetic joint replacement. A deformed hip joint does not have the ability to auto-correct the deformity of its anatomy. The elimination of the deformity of the hip joint after LCPD implies the use of therapeutic "synthetic morphogenesis". A conceivable contributor to this therapeutic synthetic morphogenesis is the osteoplastic envelope, the periosteum and the former growth zone of the articular cartilage of the proximal part of the femur and the acetabulum. A revival of the morphogenetic potential of the osteoplastic envelope in adult age would necessitate gene therapy of chondrocytes and bone cells. Cartilage does not have any blood vessels and its intercellular matrix is too dense to allow effective gene therapy. The matrix must be made less dense by using synthetic enzymes, specifically designed for the purpose, which in a reversible manner break chemical bonds within the intercellular matrix of the articular cartilage allowing gene vectors to reach the chondrocytes. To provide the guidance required by the therapeutic synthetic morphogenesis is a challenge.
"The new overthrows the old"
Legg-Calvé-Perthes' disease (LCPD) has an unknown etiology, and it cannot be prevented. Treatment (weight-relief, containment of the femoral head by the acetabulum) can often not prevent the deformity of the femoral head and the secondary deformation of the acetabulum. The affected hip joint does not have the capacity to auto-correct the deformity, it is permanent. This deformity predisposes to a reduced function of the hip joint with pain and future arthrosis (osteoarthritis) which may make a prosthetic joint necessary.
The deformity of the hip joint consists of two parts, the "redundant volume", the volume that is located outside the normal anatomy, and the "deficit volume", the volume that is lacking compared to the normal anatomy. The elimination of the redundant volume would necessitate resorption of bone tissue and the elimination of the deficit volume would necessitate growth of bone tissue. These two processes, growth and resorption, must be coordinated to achieve the normal anatomy of the hip joint and it is this coordination in time and space which poses a challenge. There are 12 principles, "modules", of morphogenesis if mesenchyme and epithelial tissues are included: Proliferation, elective cell death, migration, directed migration, aggregation, mesenchyme-to-epithelial transition, sheet folding, sheet joining, convergent extension, tubulogenesis, branching and epithelial-to-mesenchyme transition (32). Resorption of bone tissue corresponds to elective cell death and growth of bone tissue corresponds to proliferation.
To accomplish this growth and resorption of bone tissue the first structure which comes to mind is the "osteoplastic envelope" (1), the periosteum and the growth zone of the articular cartilage (2) which are responsible for the growth of the hip joint during embryogenesis and childhood. In the adult the epiphyseal growth plate of the femoral neck and the growth plates of the acetabulum have been replaced by bone. During growth the expansion of the hip socket is caused by interstitial growth within the triradiate part of the cartilage complex. The depth of the acetabulum increases during development as the result of interstitial growth in the periphery of this cartilage, and of periosteal new-bone formation at the acetabular margin. The femoral head predisposes to the concavity of the acetabulum (3). The groove of Ranvier, possibly responsible for the transverse growth of a growth plate, is present at growth plates in general (4). In order for the osteoplastic envelope to initiate the necessary resorption and growth of bone tissue the relevant genes have to be activated, that is, a gene therapy of the osteoplastic envelope has to be performed.
The articular cartilage does not have any blood vessels so effective gene therapy cannot be performed; the intercellular substance is too dense (5, 33). For gene therapy of the articular cartilage to be possible the intercellular substance has to be made less dense by breaking chemical bonds using enzymes. If the articular cartilage is to be made less dense its volume must increase. The breaking of chemical bonds has to be reversible to prevent permanent damage to the articular cartilage.
The principal candidate in articular cartilage to have chemical bonds broken is the collagen network. Collagen in cartilage is mostly of type Ⅱ. That permanent damage to the articular cartilage must be avoided means for example that chondrocytes must not escape from the collagen network and that it must be possible to re-adapt the ends of the collagen molecule so that the re-creation of the chemical bond by another synthetic enzyme can be performed. The glycosaminoglycans in the cartilage matrix have negative charges giving rise to osmotic pressure. This gives the cartilage a tendency to swell, this force is opposed by the collagen network. The synthetic enzymes must be administrated intraarticularly with the consequence that permanent damage to the synovial membrane and transfer to the systemic circulation via the synovial membrane must be avoided. It would be helpful to have a detailed 3D-picture of the molecular structure of articular cartilage which you could rotate around three orthogonal axes to better understand which chemical bonds ought to be broken to make it possible for the vectors to reach the chondrocytes, to specify the paths/tunnels to be used ("pathfinding").
Growth of the diameter of the femoral head has been studied in Chinese children (6). From this study an increase of the radius of the femoral head by approximately 2.5 mm/year can be calculated. To bridge a deficit distance of 4 cm would take 40 mm/(2.5 mm/year) = 16 years. For the purpose of NEE this growth velocity of the articular cartilage is low. A normalization of the anatomy of the hip joint implies an increase/normalization of leg length. Vessels, nerves, and tendons have to adapt to that. (Prosthetic hip joint replacement may cause damage to the sciatic nerve with an incidence of 1-2%). The femoral head comprises about two-thirds of a sphere, but these two-thirds are not perfectly spherically shaped (7). If the treatment is instituted at an age, 16-18 years, when the epiphyseal growth cartilages have been replaced by bone, a complicating factor in the form of growth from these growth cartilages do not have to be considered but instead the hormonal environment of the adult has to be considered.
Directed enzyme evolution uses repeated mutations of wild-type enzymes producing up to at least thousands of clones which are subjected to high-throughput screening (9). Directed evolution does not require a thorough understanding of the relation between structure and function. Such an understanding is necessary in rational protein design. Examples of physical theoretical methods used in rational protein design are molecular dynamics, Monte Carlo simulation and quantum mechanics.
Directed enzyme evolution of an already existing enzyme, a wild-type enzyme, has the aim to improve qualities of the enzyme such as catalysis velocity, selectivity, temperature optimum, temperature robustness, robustness against proteases, improvement of pH-profile, pH-stability, robustness against toxic products and inhibitors in raw materials. As for the development of an enzyme that catalyses a completely new chemical reaction, a citation is appropriate (9): "The development of procedures to engineer new active sites capable to efficiently catalyse reactions totally unrelated with those catalysed by natural enzymes will have an enormous impact in biotechnology and our understanding of enzyme catalysis". The construction of a new enzyme from scratch is called "de novo design" (10).
In the context of NEE the purpose is not to catalyse chemical reactions in a solution but to break chemical bonds in a dense tissue, the articular cartilage, to allow for gene vectors to reach chondrocytes and thereby to make gene therapy possible. Because the collagen molecule is embedded in the tissue the task will be more difficult. The part of the collagen molecule to be fitted to the active site of the enzyme may be blocked by the tissue. The breaking of chemical bonds must be reversible, and the re-creation of the chemical bonds is to be performed by other synthetic enzymes the action of which, as regards the end result, is the reverse of the synthetic enzymes that broke the bonds.
Examples of enzymes constructed by directed enzyme evolution are anticoagulant enzymes, procoagulants, Neprilysin and human kallikrein for the treatment of Alzheimer's disease, BoT/A for the treatment of neuromuscular disorders, Kumamolisin for the treatment of coeliac disease, tryptophan synthase, stereoselective enzymes, Rubisco, unspecific peroxygenase, and phytase. A problem sometimes encountered is immunologic reactions (9).
Collagenases that belong to the matrix metalloproteinase (MMP) family (MMP-1, MMP-8, MMP-13, MMP-18, MMP-2 (gelatinase A) and membrane-type 1-MMP(MMP-14)) break down collagen in vertebrates at neutral pH. MMP-1 preferentially breaks down type Ⅲ collagen, MMP-8 preferentially breaks down type Ⅰ collagen and MMP-13 preferentially breaks down type Ⅱ collagen, the collagen type that is most abundant in articular cartilage. They can be inhibited by TIMPs (tissue inhibitor of metalloproteinase). The triple-helical collagen is too broad to fit into the active site of the collagenase MMP-1. The enzyme first unwinds the triple-helical structure of the collagen locally before it hydrolyses the peptide bonds and produces the 3/4 and 1/4 fragments of the collagen molecules (9). MMP-1 in the first place cleaves the αⅡ(1) chain of type Ⅰ collagen and then the other two chains. These enzymes cleave the three α-chains of collagen next to the amino acid Gly in the sequence (Gln/Leu)-Gly#(Ile/Leu)-(Ala/Leu) (# shows the bond that is cleaved) about three quarters from the N-terminus of the collagen molecule. These 3/4 and 1/4 fragments denature at physiologic temperature and are degraded by gelatinases and nonspecific proteinases (in the context of NEE this problem must be addressed as the breaking of bonds in the articular cartilage has to be reversible and permanent damage to the articular cartilage must be avoided). A typical collagenase is secreted as an inactive proenzyme which consists of a propeptide (the propeptide is lost during activation), a catalytic domain, a short linker region which has a high content of proline and a C-terminal hemopexin (Hpx) domain. The Hpx-domain is responsible for the local unwinding of the collagen triple-helix.
Cathepsin K is a member of the papain superfamily of cysteine proteases. It can cleave the collagen triple helical fibrillar collagens at multiple sites different from the site cleaved by collagenases. It acts at acidic pH (ref: 12). It can cleave the telopeptides (extrahelical regions) of collagen type Ⅱ which results in the depolymerization of the collagen fibril and at a site which is located 58 residues from the N-terminus of the triple helix.
An enzyme can have more than one active site and can have promiscuity regarding selectivity (21). At the leading end of the enzyme there could be an active site which broke all the kinds of bonds which need to be broken on its way to the chondrocyte and at the rear end of the enzyme there could be another active site which mended the broken bonds. Attached to the middle of the enzyme there could be a vector carrying the nucleotide sequence to be transported to the nucleus of the chondrocyte and the rest could be broken down by intracellular enzymes. The enzyme could be a monomer so that it occupied less space.
"Synthetic biology" (13) implies a biology which has been modified by the insertion of nucleotide sequences in the genome performing specific functions which are invented by the researcher. It involves among other things the parts (promotor, operator, ribosome binding site, protein coding sequence, terminator, counters, etc), devices (logic gates such as AND, OR, NOT, negated gates, cell signalling senders and receivers, etc) and systems (feedback loops, switches, oscillators, counters, etc) approach, the BioCAD concept, cybernetics, signal theory/signal processing and systems and control theory. Examples of more ambitious topics are synthetic genomes and synthetic cells ("synthetic life"). The ideas in synthetic biology are influenced by engineering and electronics. The created functions are "orthogonal", which means that they are not interfering with the cells' normal functions. Mathematical modelling ("in silico testing", "dry lab") is important in synthetic biology. An application of synthetic biology is "synthetic morphogenesis". As mentioned above a "part" in the form of a counter has been invented, but not a timer with the ability to measure time in years and months. Such a timer could be useful in the context of NEE to define the time the synthetic morphogenesis would be operative, if that is not defined in the morphogenetic mechanism (system) itself.
To create the normal anatomy of the hip joint when LCPD has deformed it a guiding mechanism for morphogenesis is needed. As for an external source of guidance an MR-scan or CT-scan can produce an 3-dimensional image of a normal or deformed hip joint but you cannot reverse the process, i.e. you cannot program a 3-dimensional image of a normal hip joint in the computer and project a magnetic or X-ray field with that shape onto a patients deformed hip joint and use this field as a guidance to the synthetic morphogenesis to create a normally shaped hip joint.
Guidance in morphogenesis involves targeting. Considering targeting in a medical context the first thing that might come to mind is radiation therapy of cancer using several beams of X-ray or gamma rays focused at the area to be destroyed but to use several focused beams of X-ray or gamma rays with photoswitches as an intermediate link as an external source of guidance in the treatment of the deformity of the hip joint after LCPD (optogenetic orthopaedics) is not an attractive and realistic idea.
The opposite of an external source of guidance in synthetic morphogenesis is an internal source of guidance. Embryonic stem cells can have an "intrinsic positional memory" (15). Three models in morphogenesis are the morphogen hypothesis, the polar coordinate model, and the boundary model (16). The Spemann-type organizer helps to organize a midline in the AP-axis (Anterior-Posterior axis), necessary to provide a ventro-dorsal axis orthogonal to the AP-axis. The Nodal/Lefty2 system distinguishes between left and right (17). The work to construct the formalism of the concept of a "morphogenetic field" is in progress (16).
A.M. Turing invented the reaction-diffusion theory (18). Morphogens are produced in specific areas and diffuse out in the vicinity and cause growth. An "organizer" or "organizing region" is a region in an organism which can have a long-range activation combined with a short-range inhibition of the creation of another organizing region/other structures. The influence is mediated through diffusing morphogens. Hydra is a model organism for this (19).
Bone is a mineralized tissue and diffusion cannot take place in bone. To achieve something corresponding to an organizing region in a dense tissue would be to inject an amount of appropriately gene-manipulated bone cells in the centre of the future femoral head where these injected bone cells would grow to a sphere, a femoral head, replacing the surrounding tissue and the growth would stop at a suitable moment. If the centre of the femoral head of the normal anatomy is located outside of the deformed anatomy a repeated process would be necessary. To construct an "organizing region" in the articular cartilage would be problematic but perhaps necessary.
In Synthetic Duo there is no external guidance for the synthetic morphogenesis. The information necessary for the synthetic morphogenesis is inherent in the nucleotide sequence which is inserted into the chondrocytes. This nucleotide sequence will be transcribed and translated to proteins which will initiate the mechanism that will lead to the normal anatomy of the femoral head and of the acetabulum. To define this mechanism is an unsolved problem. There is no practical possibility to use an external guiding system for the synthetic morphogenesis. The guiding system must be inherent in the nucleotide sequence.
The whole of the deformity of the hip joint will not be corrected by the Synthetic Duo, only the part which is covered by articular cartilage, but that is also the most important part of the hip joint. To involve the part of the deformity which is located within the joint capsule but not covered by articular cartilage would necessitate gene therapy of bone cells at the boundary of the relevant bone tissue, perhaps through the periosteum, if there is any ("Synthetic Duo de luxe").
In an advancing motif, elimination of deficit volume, the gene therapy will cause growth of the articular cartilage. If nothing happens at the cartilage-bone interface the articular cartilage will get thicker and thicker. An activity is needed at the cartilage-bone interface and that activity is calcification of the basal layer of the articular cartilage and its transformation to bone tissue in order for the articular cartilage to have its thickness constant and the bone anatomy to be restored to normal. The bone cells have to be made to react in an appropriate manner to achieve this and this would necessitate some sort of signalling to the bone cells coordinated with the growth of the articular cartilage.
For a retreating motif, elimination of redundant volume, bone tissue underlying the articular cartilage must be resorbed and the bone cells underlying the articular cartilage must react accordingly. This too would necessitate some sort of signalling to the bone cells as part of the coordination between growth and resorption of bone tissue. There will also be some tension in the articular cartilage as the anatomy changes and this tension in the intercellular matrix of the articular cartilage must be alleviated by the chondrocytes through remodelling. (Dynamic shear strain stimulates collagen synthesis two-fold more than proteoglycan synthesis (34)).
On a strictly theoretical level, but not on a practical level, there are three principles to correct a deformity of the hip joint after LCPD:
1. Internal reference-form. The starting-point is a picture from Arthur W. Ham's "Histology" (20) which shows a decalcified femur which has been tied into a knot. Bone is a two-phase system, it consists of organic matrix and mineral, calcium hydroxyapatite. Decalcified bone is elastic but not plastic, you cannot shape it like modelling clay. The idea would be to perform an in vivo decalcification of the hip joint by the establishment of a separate external vascular system to the hip joint using erythrocytes or perfluorocarbons as oxygenators and a chelator, EDTA, to decalcify the bone tissue. Apply an internal reference-form the inside anatomy of which equals the normal anatomy of the proximal part of the femur and a separate internal reference-form for the acetabulum. Press the proximal part of the femur into the reference-form so that it acquires the normal anatomy and the corresponding procedure for the acetabulum. Re-establish the normal vascular circulation and let the hip joint recalcify after which the internal reference form is removed surgically or is resorbed.
Organic bone matrix is elastic, not plastic. It is not possible to press a decalcified proximal part of the femur into a reference form and to get the normal anatomy of the proximal part of the femur. There would also be increased pressure within the tissue and the circulation would be compromised, a new ischemia and necrosis would follow. It is possible to establish a separate external vascular system to the liver and perfuse it with cytostatica in the treatment of metastases from a malignant melanoma but to establish a separate external vascular system to the hip joint would be practically impossible. Leakage of chelator to the systemic circulation can cause hypocalcaemia which might be lethal.
Still using an internal reference-form the principle can be modified. Perform a surgical removal of the redundant volume of the deformity. Fill the deficit volume with a substance containing growth factors which will stimulate the adjacent bone tissue to growth, eliminating the deficit volume of the deformity. To have a normal articular cartilage would be a big problem.
2. Optogenetic orthopaedics. Optogenetic orthopaedics uses gene therapy, promotors, to initiate growth/resorption of bone tissue to attain the normal anatomy, all regulated by external beams of X-rays or gamma-rays. A conjugate is injected in the systemic circulation or intraarticularly. A conjugate consists of two scintillators, S1 and S2, two photoswitches, P1 and P2, a cell entry function and a promotor. There are two sets of beams, B1 and B2, with different frequencies. B1 will activate S1 but not S2 and this scintillator, S1, will activate its own photoswitch, P1. B2 will activate the conjugate's other scintillator, S2, but not S1, and this scintillator will activate its own photoswitch, P2. Both P1 and P2 of the conjugate have to be activated at the same time for the cell-entry function to be activated and this only happens at the focus of the two sets of beams B1 and B2. When the growth/resorption of bone tissue has been ongoing for a while and a re-evaluation is necessary to decide where growth and resorption are necessary from that time onwards, the process is stopped by the injection of a detaching molecule which will remove the inserted promotors in the chondrocytes and bone cells and the process is repeated. Optogenetic orthopaedics is a step-by-step treatment, and the summation of the steps will result in the normal anatomy of the hip joint.
This elaborate system with two sets of beams and conjugates containing several components, used in a step-by-step fashion is a bit too elaborate and unrealistic.
3. Synthetic Duo. Synthetic Duo requires that you assume the role of God Almighty because you have to give the hip-joint the ability to auto-correct its own anatomy and there is no mammal where a hip-joint has that ability. Up to now, there has been no orthopaedic surgeon who has claimed that he is God Almighty, at least no one with a confirmation by the Pope. Synthetic biology with its application synthetic morphogenesis is used. A vector, administrated intraarticularly, brings a nucleotide-sequence into the chondrocytes, initiating transcription and translation of proteins the interactions of which constitute a morphogenetic continuous (not a step-by-step) mechanism (system) that will cause growth/resorption of bone-tissue at relevant places, resulting in the normal anatomy of the hip-joint. Unfortunately, such a morphogenetic mechanism does not exist, and it has to be invented. What is the connection between a sphere and a nucleotide sequence?
There are no vessels in articular cartilage and that prevents effective gene therapy to be performed. To make effective gene therapy in articular cartilage possible the intercellular substance has to be made less dense by using synthetic enzymes, either developed by directed enzyme evolution (collagenases, cathepsin K, enzymes cleaving glycosaminoglycans) or rational de-novo design. The breaking of chemical bonds must be reversible to prevent permanent damage to the articular cartilage. A set of synthetic enzymes to break the appropriate chemical bonds and another set of synthetic enzymes to re-create the same chemical bonds and in between the gene therapy. All these three sets of substances administrated by intraarticular injections. Theoretically, the enzymes re-creating the broken bonds could be replaced by a DNA-sequence coding for them administrated at the same time as the DNA-sequence responsible for the synthetic morphogenetic mechanism and activated after this mechanism has reached its goal. This would make a third intraarticular administration (injection) unnecessary.
When contemplating the therapeutical normalization of the anatomy of the hip joint after LCPD, this is what you finally arrive at: A combination of synthetic enzymes and synthetic morphogenesis. In internal reference-form the guidance of the synthetic morphogenesis is located internally, the internal reference-form has an internal anatomy equivalent to the normal anatomy of the hip joint. In optogenetic orthopaedics the guidance of the synthetic morphogenesis is located externally through the sets of focused beams of radiation. In Synthetic Duo, the location of the guidance of the synthetic morphogenesis has again been shifted from an external source to an internal source, the DNA-sequence of the gene-therapy.
As a first preliminary working model for the Synthetic Duo might be used the following five-point schedule:
*** 2022 , 2024 ***
In the Crackpot´s workroom in the cellar there was a human skeleton located on a chair at the desk opposite the Crackpot's desk. The Crackpot had been told that the skeleton belonged to an orthopaedic surgeon who had worked at the hospital before the Crackpot began there. The diseased orthopaedic surgeon, Dr. Primus, had worked on a problem for decades but could not solve it. There was a cemetery at the hospital but because of one reason or the other the hospital had forgotten to bury him. It was not until later that the Crackpot found out that the diseased orthopaedic surgeon had worked fifty years on the same problem as the Crackpot himself, LCPD. Dr. Primus tried to find the cause of the disease but failed. He proposed several hypotheses but none of them could be proved. The Crackpot explained why it was impossible to find the cause of the disease, the impossibility to perform an ACPS-measurement. Instead of making a meaningless effort to find the aetiology of the disease the Crackpot used his six-point approach: The first point was the realization that it was impossible to find the aetiology of the disease because it was impossible to perform an ACPS-measurement. The second point was to take the consequence of point number one i.e. to direct the interest to the deformity itself, to treat the deformity in such a way that it disappeared. The third point was to put forward proposals of strategies to accomplish this effective treatment of the deformity of the hip joint caused by LCPD: internal reference-form, optogenetic orthopaedics and the synthetic duo. It had taken a long time for him to come up with these three proposals but it was no surprise that he had managed to do so because apart from being a physician he also had a MIS-degree (Master of Impossible Strategies) from Oxford University. The fourth point was to choose among the proposals the strategy which was deemed to be the best one, in this case the third one, i.e. synthetic duo. The fifth point was to estimate how long a time this project would take and his estimate was that it would take about four thousand years and that he was no. 2 in a succession of 4000/50 = 80 doctors who would work with this problem, each for fifty years. The sixth point was to realize this third alternative and to put it into clinical practise. He understood that there would be a lot of skeletons that would pile up in his workroom in the future. There were some of his patients who were puzzled when they were asked to come back for a new appointment in 4000 years to get their hip joint´s anatomy corrected. To have a check-up in a year was acceptable but to wait for 4000 years they thought was too much.
The Crackpot often wondered why he himself was so advanced and everybody else so primitive. He was influenced by the birth of the sheep Dolly on 5 July 1996 using the process of nuclear transfer (1,2). The nucleus from a mammary gland cell of a grown-up sheep was injected into an enucleated egg cell from another sheep which thus was serving as a cytoplasmic donor. The cell division was initiated by a direct electric current and the blastocyst was inserted into a surrogate ewe. The birth of Dolly proved that the nucleus from a cell from a grown-up animal had the potential to provide the necessary genetic material for a new individual including joints, the nucleus was totipotent. He speculated that it in the far future would be possible to transform a joint with severe arthrosis with obliterated articular cartilage, bone cysts and osteophytes to a normal joint with no signs of arthrosis. He speculated that this technology also could be applicable to trauma, cancer surgery and congenital malformations. He wanted to preserve the original normal tissues of the human body. Therefore, he wanted to be able to treat osteoarthritis in a way that restored the joint to normality without the horrendous presence of a prosthetic joint made of metal and plastic. This was contrary to what Napoleon strived for. Napoleon loved prosthetic joints. When discussing prosthetic joints the Crackpot vividly and shocked described how prosthetic joint surgery was carried out with a power saw, a crowbar, dynamite, nuclear devices, a pneumatic drill, a sledge hammer and two stoned orthopaedic surgeons inclined to violence, and he wondered how on earth such a brutal procedure ever could have found its way into medicine. There were those who said that the Crackpot's ideas were unrealistic but he waved aside these objections and said that he did not have to pay any attention to less knowledgeable people.
Napoleon often wondered why he himself was so advanced and everybody else so primitive. The mainstream approach to diseases was to try to find the aetiologies and to establish treatments for them but this was something which took too long a time and often was impossible. According to Napoleon the correct approach was to shift focus from diseases to the human being itself and to transform it to something less amenable to disease. This is the reason for his research in robots and he had had some success in the 3D-printing of orthopaedic surgeons. The Crackpot's idea of the orthopaedic field theory was an extreme idea and Napoleon also had an extreme idea and that was to make a digital copy of the human brain and to let this digital copy live its life in a computer. In this way you would get rid of the human state which always was afflicted by disease. The human state itself is the culprit and has to be abandoned. It has had its day. It is not tenable any longer. He thought that doctors had gotten hold of the wrong end of the stick and that it was his mission to remedy this because it was only he who had the superior intellect which the mission demanded. Napoleon's first interest was prosthetic joints, he then moved on to robots and his final goal was to digitize the life of every individual in a computer. Prosthetic joints - robots - the digitization of the life of every individual in a computer, this was Napoleon's strategy.
The possibility of the mankind living their lives in a computer is mentioned in "Physics of the future" by Michio Kaku (3). A citation from the text: "In the ultimate scenario, we discard our clumsy bodies entirely and eventually evolve into pure software programs that encode our personalities. We "download" our personalities into a computer. If someone presses a button with your name on it, the computer behaves as if you are inside its memory since it has encoded all your personality quirks inside its circuits. We become immortal, but spend our time trapped inside a computer, interacting with other "people" (that is, with other software programs) in some gigantic cyberspace/virtual reality. Our bodily existence will be discarded, replaced by the motion of electrons in this gigantic computer." This topic has also been explored by National Geographic's TV-series "Year Million" (4).
When Napoleon read the cited text and watched the TV-series he got overjoyed. To live one's life in a computer where there were no diseases, what a wonderful idea! He imagined how he would have an external hard-disk containing the whole mankind, all in his possession. He would have achieved world dominion. He took the globe on his desk and embraced it lovingly. The whole world would be his. Only his! "Greatness is my hallmark, I will prevail". There were those who said that his ideas were unrealistic but he waved aside these objections and said that he did not have to pay any attention to less knowledgeable people.
The Crackpot and Napoleon can be compared with each other using the dialectic method used by the German philosopher George Wilhelm Friedrich Hegel when describing the evolution of history (5). First, society is arranged according to certain chosen principles, the "thesis". After some time, dissatisfaction with these principles grows into a revolution against them and opposite principles are chosen to form the society, the "antithesis". After some additional time and the insight that this antithesis also is unsatisfactory elements from both the thesis and antithesis are combined into a "synthesis", a society which is satisfactory.
The "thesis" is here represented by the Crackpot who advocates the normal human state including any treatment which preserves it, and rejects synthetic prosthetic joints. The opposite to this, the "antithesis", is represented by Napoleon who rejects the human state, favours synthetic prosthetic joints and advocates robots and digital existence in a computer instead of human beings of the ordinary category. By combining elements from both the thesis and antithesis a "synthesis" results, here represented by present day orthopaedic surgery which tries to treat local defects in articular cartilage by biological means, i.e. to preserve the normal human state but at the same time inserts synthetic prosthetic joints, i.e. has an acceptance of the fact that the human state has its flaws. The Crackpot and Napoleon are exact opposites of each other. As for German philosophers, both the Crackpot and Napoleon had read Friedrich Nietzsche and each one of them considered himself to be far superior to everybody else.
Introductory explorations (optogenetic orthopaedics).
A new concept is introduced, noninvasive envelope engineering (NEE), which denotes the coordinated growth and resorption of bone tissue from the periphery of the proximal portion of the femur and from the acetabulum in order to eliminate the whole of the deformation of the hip joint in the adult patient which often is the result of Legg-Calvé-Perthes' disease (LCPD). The tissue component responsible for the coordinated growth and resorption is the osteoplastic envelope, the periosteum and the articular cartilage, and is initiated, maintained and terminated by the necessary genes in sequential stages. As a first devised principle, presently the only one imaginable, of substituting the guiding mechanisms of morphogenesis an elementary scheme of synchrotron radiation with predefined wave length and doses calculated with Monte Carlo methods, scintillators and photoswitches enabling the required genes/gene promotors to enter the cells in the required areas is described in a broad outline. A theoretical analysis is presented with no references to any experimental work carried out specifically aimed at NEE. Because of the special character of the problem, involving overcoming major obstacles such as constructing a targeting system with rays of ionizing radiation and a conjugate consisting of a scintillator and a photoswitch on a microscopic level, gene therapy in articular cartilage, substitution of morphogenesis including its fine-tuning of the anatomy of the hip joint, keeping the effects of the conjugates targeted in space and time, the hazardous effects of ionizing radiation, cellular senescence and low growth velocity of the articular cartilage, NEE seems to be like an unreachable star in heaven and a suitable time lapse to the next evaluation of the possibilities of NEE has been set to a thousand years.
Key words: Legg-Calvé-Perthes' disease (LCPD), noninvasive envelope engineering (NEE), redundant volume, deficit volume, motifs, the osteoplastic envelope, synchrotron radiation, Monte Carlo transport of radiation, scintillators, photoswitches, remote control of gene therapy in tissue engineering, stem cells, cellular senescence, temporal category persistence (TCP), the algorithm, the menu of impossibilities, the ACPS-measurement, the trinity of LCPD.
1.Introduction
2.Noninvasive envelope engineering (NEE) - Outline
3.Anatomy
4.Histology. The four motifs
5.Growth factors and growth velocities
5.1.Growth factors
5.2.Growth velocities
6.The articular cartilage
6.1.Structure and permeability
6.2.Senescence
7.Gamma radiation and X-rays
7.1.Physics
7.2.Radiobiology
7.3.Radioprotectors
7.4.Radiotherapy
7.5.Monte Carlo transport of photons and electrons
7.6.Synchrotrons and synchrotron radiation
7.7.Synchrotron radiation in medicine
7.7.1.Minibeams
7.7.2.Microbeams
7.8.Scintillators
7.8.1.Introduction
7.8.2.Inorganic scintillators, ceramic scintillators, thin film scintillators
7.8.3.Organic scintillators
7.8.4.Nanocomposite scintillators
8.The conjugate: The beam-photoswitch configuration and mechanism of activation
9.The focus: Direct points and indirect points, boundary points and internal points
10.Photodynamic therapy
11.Phototriggers
12.Photoswitches
13.Transport: Radiation, blood flow, diffusion in
articular cartilage, intracellular transport
14.Genes
14.1.Gene control
14.2.Optogenetics: Switchable gene promoter systems
14.3.Gene therapy and gene delivery systems
14.3.1.Introduction
14.3.2.Viral vectors
14.3.3.Nonviral vectors
14.4.Gene therapy in bone and articular cartilage
14.4.1.Electroporation
14.4.2.Viral vectors
14.4.3.Synthetic enzymes
14.5.Ionizing-radiation-responsive compositions
15.Signalling pathways: the ON-OFF and the wave length/polarization puzzles
16.Moulding and the algorithm
17.The menu of impossibilities
18.Concluding remarks.
19.3D-printing.
20.References
"You have to open a second front"
Josef Stalin
Without a linkage analysis it is impossible to determine the aetiology of the disease. The reason for this is that it is impossible to perform a continuous ACPS-measurement (Anatomy, Circulation, Pressure, Strength) in every point of the femoral head shortly before and during the beginning of the disease. Such a continuous ACPS-measurement could in theory answer the critical question: What comes first, the fracture or the ischemia? X-rays, CT-scans, MR-scans, ultrasonography scans and examination of histologic specimens cannot answer this question. This is an example of the basic principle of cause-effect applicable to all sciences. Is the fracture the cause and the ischemia the effect or is the ischemia the cause and the fracture the effect? It may also be impossible to determine the aetiology of the disease with a linkage analysis.
In Japan there has been identified a gene mutation in collagen in a family with an autosomal dominant hip disorder manifesting as LCPD (1). The majority of patients with LCPD do not have that particular mutation (2). An example of a genetic disease with a mutation in collagen encoding genes resulting in impaired strength of skeletal tissue is osteogenesis imperfecta. There are various mutations in different locations in the genes coding for collagen that can cause this disease and not only a single one (3). The same principle applied to LCPD would make the disease a result of impaired strength of the skeleton, perhaps because of retarded mineralization (reduced skeletal age). Caffey (4) observed a fracture in the femoral head visible on the Lauenstein projection (flexion and abduction in the hip joints) of the X-ray as the first visible sign in the early stage of the disease. He proposed that the fracture comes first and the compression of bone tissue including vessels and ischemia afterwards, not the other way round. The question is complicated by the fact that there are plain radiographs showing no deformation but an increased density of bone tissue as a sign of ischemia but a plain radiograph is a projection and does not show the whole three-dimensional surface.
This would make the aetiology of LCPD an example of a combination between heredity and environment. In this case the environmental factor is the gravitational force. This also makes the aetiology a stochastic phenomenon. With the disease gene present some of the children will, because of high enough physical stress on the hip joint, get a fracture in the femoral head (or both, 10-15%) because of the impaired strength of the skeleton. It is a matter of pure chance, depending on how physically active they are. This combination of heredity and environment may make it difficult to establish a distinct mode of inheritance.
It also raises the question whether a genetic predisposition is required for LCPD in all cases or if the environmental factor is enough, i.e. if high physical stress is enough to cause a fracture in the femoral head in a percentage of the patients, in that case the search for the aetiology will go on indefinitely and nothing except from physical stress will be found. At birth there is no certificate attached stating that provided there are no mutations there will be no fracture of the femoral head, visible only on the Lauenstein projection, during childhood. Children can get a fracture of their distal radii without any other cause than physical stress, not everybody, but some will and that is inevitable.
Regarding the treatment of the deformation of the hip joint caused by LCPD with the aim of the establishment of the normal anatomy, the first generation of principle1 is to accomplish this by surgery at one or more occasions. The deformation of the hip joint (femoral head, femoral neck and the secondary deformation of the acetabulum) after LCPD consists of two parts, the "redundant volume" and the "deficit volume". The redundant volume is the volume outside the normal anatomy and the deficit volume is the volume which is lacking compared to the normal anatomy. The redundant volume is removed through surgery, the deficit volume is filled with a resorbable material which will stimulate the borders of bone tissue to invade and replace it with normal bone tissue. The procedure will necessitate the use of a "reference form" the inside anatomy of which is equivalent to the normal anatomy, apart from the thickness of the articular cartilage, both for the proximal portion of the femur and for the acetabulum, which will cause an obvious problem if one tries to insert the reference form for the proximal part of the femur into the reference form for the acetabulum. The reference form will also cause problems when explaining how the articular cartilage can be formed when deprived of intermittent pressure. The reference form is resorbable or removed at a later occasion. The articular cartilage of the femoral head and of the acetabulum, hyaline in nature, not fibrillar, is restored on the whole of the two articular surfaces, not only in a localized, limited area. As for the articular cartilage an alternative could be the insertion of a 3D-printed articular cartilage (5). Attention is given to the vascularization and circulation, a new ischemia must be avoided as well as infection. The distance that has to be bridged by vascularization could be reduced by a vascularized bone-muscle graft. These principles are on the whole in mainstream research, "tissue engineering", repairing localized defects in the articular cartilage of the knee by injecting cultivated chondrocytes under a transplanted sheath of periosteum, the search for biodegradable materials to replace autologous bone transplants from crista iliaca and the frustration at being able only to cultivate cells and smaller aggregates of tissues and not whole organs with intact vascularization, derived from stem cells from the patient to avoid immunological rejection, to be transplanted to patients. If a complicating factor in the form of growth in the epiphyseal growth plate is to be avoided the treatment should be given after the closure of the epiphyseal growth plate.
The second generation of principle of treating the deformation of the hip joint after LCPD, "noninvasive envelope engineering", rests on the fact that the cells in the osteoplastic envelope, the periosteum and the articular cartilage, do not lose their nuclei when the growth has ceased, i.e. all the genes which together constitute the genome are still there. The osteoplastic envelope has created the hip joint.
A theory for a third generation of principle of treatment with the same aim as the first and second generations, the normalization of the anatomy of the hip joint after LCPD, will probably never arise. There are mechanisms producing excellent results concerning hip joint anatomy, and anatomy of the body as a whole, morphogenesis (6,7), but these mechanisms have never been designed to correct a deformation of a hip joint after LCPD and in the adult it is all shut down.
The long bone of the thigh, the femur, has not only grown along its length axis but also in a plane perpendicular to its length axis. This is the starting point for a tentative line of thought regarding the treatment of the deformation after LCPD which exploits the fact that bone is a living tissue with living cells. The deformation of the hip joint (femoral head, femoral neck and the secondary deformation of the acetabulum) after LCPD consists of two parts, the redundant volume, the volume outside the normal anatomy, and the deficit volume, the volume which is lacking compared to the normal anatomy.
During growth the increase in width of the femoral head and of the femoral neck is accomplished by "the envelope", proliferating chondrocytes in the articular cartilage and osteoblasts in the mesenchymal tissue corresponding to the periosteum lining the femoral neck.
NEE is a step-by-step treatment which consists of remote control of gene therapy in tissue engineering in bone and articular cartilage where the remote control is achieved by the targeting of two sets of beams of ionizing radiation, B1 and B2, where each set of beams activates its own scintillator because of the frequency of the beams. The two sets of beams, B1 and B2, are switched on at the same time or not, depending on whether there is a need for a minor time interval in order to allow for the removal of secondary physical effects of the radiation before the next set is switched on. Each scintillator is coupled to its own photoswitch. A photoswitch will be activated by the energy delivered by its scintillator which in turn is activated by its set of beams due to the frequency of the beams. With the use of the two sets of beams of ionizing radiation where each set of beams activates only its own scintillator and photoswitch, activated conjugates able to enter the cells and their nuclei will only occur at the focus of the two sets of beams and not along the entire paths of the beams. A conjugate consists of six components, two scintillators, S1 and S2, two photoswitches, P1 and P2, a cell entry function and a promotor which will attach to its intended site in the genome. This promotor is detachable through the influence of a detaching molecule. The scintillator S1 is coupled to the photoswitch P1 and the scintillator S2 is coupled to the photoswitch P2. For the cell entry function to be activated both P1 and P2 must be activated simultaneously. The two sets of beams have the same focus. The ON-signal with ionizing radiation will only activate the photoswitches indirectly through the scintillators and not directly. There must be two axes, the first axis comprising beam set B1, scintillator S1 an photoswitch P1 and the second axis comprising beam set B2, scintillator S2 and photoswitch P2. Both of the 2 axes must be active at the same time in order to get an active conjugate in the focus of the 2 sets of beams. Had a principle with only one axis been used active conjugates would exist along the entire path of the beams and not only at the focus of the beams.
Each step is initiated by the intravenous or the intraarticular administration of conjugates continued by the targeted signals in the form of focused ionizing radiation and terminated by the detachment of all the conjugates through the intravenous or the intraarticular administration of detaching molecules. Each step will cause a slight reduction of the deformation of the hip joint and the combined effect of all the steps will result in the normal anatomy of the hip joint.
The articular cartilage bordering on the deficit volume is subdivided into crossfire units, CFUs, on which targeted ionizing radiation, X-ray or gamma ray, is focused using 2 or more beams in each of the two sets of beams, B1 and B2. The focused ionizing radiation in the crossfire units will activate conjugates injected intraarticularly consisting of two scintillators, S1 and S2, two photoswitches, P1 and P2, a promotor and have the ability to enter the cells and the nuclei when the two photoswitches are activated at the same time. The promotor which is a part of the conjugate will attach to its intended site in the genome and cause activation/mitosis of stem cells located superficially in the articular cartilage (there is something called "senescence" of stem cells, i.e. they cannot any longer divide but we will perform this outline in a simple and unconcerned manner).
The only way to eliminate the deficit volume when the articular cartilage borders on the deficit volume in the adult patient is to achieve this through growth in the articular cartilage. At the end of a step the promotor will be detached from the genome through the intraarticular administration of detaching molecules.
For the deficit volume lying inside the joint capsule and where the bone bordering on the deficit volume is not covered with articular cartilage and for the deficit volume outside the joint capsule, the conjugates are injected intravenously. The CFUs are directed to the border of this deficit volume where the switchable promotors (the conjugate with its six components) activate osteoblasts in the lining periosteum (cambium layer) causing synthesis of bone tissue and reduction and elimination of the deficit volume. At the end of a step the conjugates are removed through the intravenous administration of detaching molecules.
For the redundant volume lying both inside and outside the joint capsule the conjugates are injected intravenously. The function of the switchable promotors for the redundant volume covered by the articular cartilage is to activate osteoclasts from the bone underlying the articular cartilage in order to resorb the bone reducing and eliminating the redundant volume.
The function of the switchable promotors for the redundant volume not covered with articular cartilage is to activate osteoclasts from the inner layer of the periosteum and/or from the cancellous bone underlying the thin cortical bone. Targeted ionizing radiation is used to allow the conjugates to enter the cells and intravenous administration of detaching molecules to remove the promotors at the end of each step.
To avoid mixed effects conjugates with different kinds of promotors should not be present in the systemic circulation at the same time, a pause will ensure the necessary clearance of the conjugates.
NEE is the combination of a targeting system with two sets of beams and conjugates and its application area, gene therapy in bone and articular cartilage. This combination presents a series of obstacles. The first is that such a targeting system does not exist. Scintillators are used on a macro-scale, for example in high energy physics to detect particles/radiation but for NEE they would be used on a molecular scale which would mean that the absorption would be too low. It would require a very special scintillator yet to be invented.
The second obstacle is associated with the application area, articular cartilage does not have blood vessels and the intercellular substance is penetrable only for small molecules, gene therapy cannot be effectively performed in articular cartilage, particularly not in vivo.
The third obstacle is associated with the proposed principle itself, i.e. to substitute morphogenesis with remote control of gene therapy in bone and articular cartilage where the remote control is achieved by two sets of beams with X-rays or gamma-rays and conjugates in a stepwise fashion is a rude and very probably an insufficient method. The remote control would operate in a discrete way but morphogenesis operates in a continuous manner and has an inbuilt feedback system. The step by step remote control of the gene therapy could have its discrete mode of operation changed to a continuous mode of operation by making the steps smaller in time to finally be infinitely short but that would make the dose of ionizing radiation infinitely high. To try to create a substitute for the natural morphogenesis which will function in the adult patient is to have high ambitions.
The fourth obstacle is to keep the treatment targeted, i.e. there should not be any activated conjugates outside the intended CFUs, especially not disseminated throughout the whole body.
The fifth obstacle is the fact that a serious side effect of ionizing radiation is that it can cause cancer.
The articular cartilage of the acetabulum and of the femoral head are in direct contact with each other. Because it is necessary to differentiate between the redundant and the deficit volumes the cross-fire volumes of the targeting radiation must encompass only one category of volume (redundant/deficit). The cross-fire volumes must be small enough to fulfil this goal.
In addition to the redundant and deficit volumes there is a third category of volume, the intermediate volume ("the non-deformed volume") which is the part of the hip joint which does not belong to the redundant or deficit volumes. The intermediate volume plus the deficit volume equals the normal anatomy of the hip joint. The intermediate volume plus the redundant volume equals the deformed hip joint anatomy after LCPD.
The part of the articular cartilage of the femoral head which is in direct contact with the articular cartilage of the acetabulum for a given position of the hip joint belongs to one of the categories deficit, redundant or intermediate volumes. Each one of these categories can be divided into three parts depending on which category of volume of the acetabulum the articular cartilage of the femoral head is in direct contact with. Using the abbreviations "H" for the femoral head, "A" for the acetabulum, "D" for deficit, "R" for redundant and "I" for intermediate the corresponding ratios between surface areas are constructed.
"HDD", "HDR" and "HDI" are the ratios of the areas of the articular cartilage of the femoral head, belonging to the deficit volume, which are in direct contact with the acetabulum which belongs to the deficit volume, redundant volume and the intermediate volume respectively. "HRD", "HRR" and "HRI" are the ratios of the areas of the articular cartilage of the femoral head, belonging to the redundant volume, which are in direct contact with the acetabulum which belongs to the deficit volume, redundant volume and the intermediate volume respectively. "HID", "HIR", "HII" are the ratios of the areas the articular cartilage of the femoral head, belonging to the intermediate volume, which are in direct contact with the acetabulum which belongs to the deficit volume, redundant volume and the intermediate volume respectively.
"ADD", "ADR" and "ADI" are the ratios of the areas of the articular cartilage of the acetabulum, belonging to the deficit volume, which are in direct contact with the femoral head which belongs to the deficit volume, redundant volume and the intermediate volume respectively. "ARD", "ARR", "ARI" are the ratios of the areas of the articular cartilage of the acetabulum, belonging to the redundant volume, which are in direct contact with the femoral head which belongs to the deficit volume, redundant volume and the intermediate volume respectively. "AID", "AIR", "AII" are the ratios of the areas of the articular cartilage of the acetabulum, belonging to the intermediate volume, which are in direct contact with the femoral head which belongs to the deficit volume, redundant volume and the intermediate volume respectively.
From the definitions of the ratios it follows that HDD + HDR + HDI = 1, HRD + HRR + HRI = 1, HID + HIR + HII = 1, ADD + ADR + ADI = 1, ARD + ARR + ARI = 1 and AID + AIR + AII =1. High values of the ratios comprising the same category of non-intermediate volumes (redundant/deficit), that is HDD, HRR, ADD and ARR, will allow the average volume of the crossfire units to be higher which will simplify the procedure as the number of crossfire units may be lower. These ratios may change with the position of the hip joint and with time during the treatment.
The deformation (D) is defined as the sum of the absolute value of the deficit volume of the hip joint (including the proximal part of the femur and the acetabulum) and the absolute value of the redundant volume of the hip joint.
A part of the redundant volume is covered with articular cartilage. The nourishment of the articular cartilage is, apart from intermittent compression and the presence of synovial fluid, dependent on the subchondral vessels, lying beneath the articular cartilage. In this case the elimination of redundant volume will remove the bone support for the articular cartilage. The elimination of the redundant volume must be performed in such a way that the collapse of the articular cartilage is avoided. When the redundant volume of the bone tissue has been removed the articular cartilage must be firmly attached to the underlying and remaining bone tissue.
For more severe deformations a larger part of the articular cartilage belongs to the redundant volume, located medially in relation to the femoral neck, because of decreased femoral neck angle (coxa vara). The parts of the redundant and deficit volumes which are to be corrected first and which ones are to be corrected later are calculated in an optimal sequence with special attention to correcting the femoral neck angle and to keeping the articular cartilage in its right place. All of the CFUs do not have to have the ON-signal with focused ionizing radiation at the same time. The normalization of the femoral neck angle will greatly reduce the magnitude of the redundant and deficit volumes.
If larger vessels are located in the redundant volume the tissue will hopefully take care of the rearrangement of the vascular anatomy in order to prevent a new ischemia. The vascular anatomy of the proximal portion of the femur has been described by Trueta (8,9).
To completely cover a surface with CFUs it will be necessary to irradiate a part of the surface twice, it is the boundary regions between the CFUs which require special attention in this regard.
In a normal hip joint nor the femoral head nor the acetabulum has exact sphericity (10). In the book referred to the finite element method (a computerised method originally used in airplane manufacturing) is used to calculate pressure distributions. When the femoral head is deformed after LCPD the femoral head is often larger than normal ("coxa magna") (11). Elimination of the deformation of the hip joint after LCPD will result in the elimination of the leg length shortening. The joint capsule, the ligaments, muscles, vessels and nerves spanning the joint will have to adapt to the normalization of the leg length.
The development of the acetabulum has been described by Ponseti (12). The acetabulum probably has a larger deficit volume than redundant volume.
The elimination of the deficit and redundant volumes is accomplished by four different histologic processes, "motifs". The classification of these four motifs is based on the category of volume which is to be eliminated (deficit or redundant) and on existing or non-existing coverage by articular cartilage of the outward border of the existing bone. In the first two motifs the articular cartilage covers the bone, in the last two motifs it does not.
Motif number one is the elimination of the deficit volume when the articular cartilage covers the bone bordering on the deficit volume, it is applicable to both the femoral head and the acetabulum.
The only way to eliminate the deficit volume when the articular cartilage borders on the deficit volume is to initiate growth in the articular cartilage through intraarticular injection of conjugates and this in the hormonal environment of the adult where growth has ceased, indeed a science fiction theme. Chondrocytes do no lose their nuclei during the final stages of differentiation as erythrocytes and keratinocytes do. In addition, the growth velocity must be increased compared to what the articular cartilage has during growth up to the end of puberty and this is yet another obstacle. When the deficit volume bordering on the articular cartilage is eliminated the growth in the articular cartilage must stop.
Motif number two is the elimination of the redundant volume when the outward border of this redundant volume facing the articular cavity is covered with articular cartilage. This is accomplished by osteoclasts recruited from the cancellous bone adjacent to the thin corticalis, on which the articular cartilage is situated.
Motif number one and motif number two are cartilage motifs. Motif number one is an antimotif to motif number two and vice versa, motif number two is an antimotif to motif number one.
Motif number three is the elimination of the deficit volume of the femoral neck and acetabulum where the synovial lining corresponding to the periosteum, and not the articular cartilage, borders on this deficit volume. This is accomplished by osteoblasts recruited from the cambium layer of the mesenchymal lining. In the case the mesenchymal lining corresponding to the periosteum does not exist2 the alternative is to recruit osteoblasts/osteogenic cells from the adjacent cortical/cancellous bone. The cortical bone is inhabited by osteocytes.
Motif number four is the elimination of the redundant volume of the femoral head and femoral neck (proximal portion of the femur) and of the acetabulum where the outward border of this redundant volume is not covered by articular cartilage but with mesenchymal tissue corresponding to the periosteum. This is achieved by the recruitment of osteoclasts from the inner layer of the mesenchymal layer (cambium layer) and/or from the cancellous bone adjacent to the cortical bone.
Motif number three and motif number four are bone motifs (the existing bone is not covered by articular cartilage). Motif number three is an antimotif to motif number four and vice versa, motif number four is an antimotif to motif number three. Motif no. 1 and motif no. 3, both aimed at eliminating the deficit volume, are advancing motifs. Motif no. 2 and motif no. 4, both aimed at eliminating the redundant volume, are retreating motifs.
These four motifs are classified according to what is achieved from an anatomical point of view. NEE is the simultaneous realization of these four motifs in a coordinated manner. The cartilage motifs, motif number one and motif number two, seem to be the more difficult ones and they are also the most important ones in the sense that they are to ensure the spherical shape of the weight-bearing portions of the femoral head and of the acetabulum, thereby preventing future symptoms from the hip joint, provided that there already has not been inflicted any microscopical damage upon the articular cartilage by the incongruence in the hip joint which ten years later will develop into an arthrosis revealed by a plain radiograph and earlier by an NMR.
The cartilage motifs together describe a situation where different parts of the articular cartilage move in opposite directions. With respect to the femoral head the articular cartilage in motif number one moves away from the centre of the femoral head and in motif number two the articular cartilage moves towards the centre of the femoral head. The task to compensate for the strain produced in the articular cartilage in the interface produced by this relative motion is delegated to the chondrocytes through remodelling of intercellular substance. The ability to a fast remodelling in the articular cartilage is probably not large, the mean half-life of glycosaminoglycans in the human femoral head articular cartilage is 800 days (13). By the use of isotopic disappearance and autoradiography of 35SO42- and glycine-3H in the articular cartilage of the distal end of the femur of adult rabbits it was identified a metabolically fast fraction corresponding to over one fourth of the polysaccharide in the tissue having a half-life of about eight days (14). The articular cartilage has been able to adapt to the new, deformed, anatomy during LCPD, presumably the turnover rate of the intercellular substance can be increased under stress.
The classification of category of volume is made at the beginning of each step of the treatment. If a part of the deficit or the redundant volumes should change category during the treatment it will be a case of lack of "temporal category persistence" (TCP). This would necessitate the antimotif to be initiated.
With reference to these four motifs there is a wider definition of the concept of "the envelope", it comprises all the tissues directly engaged in the elimination of the redundant and deficit volumes, i.e. the articular cartilage of the femoral head and of the acetabulum, the thin cortical bone and adjacent cancellous bone underlying the articular cartilage of the femoral head and the acetabulum, the mesenchymal tissue, corresponding to the periosteum, lining the femoral neck with the underlying thin cortical bone and adjacent cancellous bone. The concept of an osteoplastic envelope was introduced by Hevelka and Horn (15), it comprises the periosteum with its associated osteoblasts and the tidemark (the tidemark is the line between the deep zone and the calcified zone of the articular cartilage (16)) with its accompanying chondrocytes. The principle of NEE is remote control of the osteoplastic envelope (noninvasive envelope engineering).
LCPD causes damage to the shape of the hip joint the normal anatomy of which has been created by the osteoplastic envelope and it is this envelope which is the tool of NEE. To treat the deformation of the hip joint one resorts to the identical structure which created the hip joint. The osteoplastic envelope has a long and proven tradition of producing excellent results concerning hip joint anatomy so to use the osteoplastic envelope in the treatment of the deformation of the hip joint after LCPD has a natural and attractive aesthetics which a prosthetic joint does not possess.
Odd numbered motifs, the advancing motifs, related to elimination of deficit volume, rely on osteoblasts ("osteoblastic predominance") and even numbered motifs, the retreating motifs, related to elimination of redundant volume, rely on osteoclasts ("osteoclastic predominance"). The engagement of one type of cell does not necessarily exclude the other kind of cell because of the coupling of the activity of osteoblasts and osteoclasts (17).
Aspects related to the articular cartilage are the function of growth mediated by the division of stem cells in the superficial zone of the articular cartilage, collagen rearrangement in order to remove tension in the articular cartilage as the shape of the articular cartilage changes because of altered anatomy of the bone, its coverage of the joint surfaces and its secure attachment to the underlying bone tissue.
A motif which uses a CFU including bone marrow would have rapidly dividing cells in the bone marrow exposed to focused ionizing radiation.
A simple and easily understood scheme of all the growth factors that exist in developing bone and articular cartilage, how they interact with each other with stimulatory, inhibitory and potentiating effects and where this scheme has reached its final and complete state which will not be added to or changed in the future and that without hesitation provides the answer to the question which growth factors/genes should be used for each of the four motifs, does not exist (7,16,18,19,117).
Skeletal biology and Medicine, Part A, published in 2007 (19) provides much information about this topic. Some facts from a selection of the articles occurring in this reference have been compiled:
BMPs. BMPs (Bone morphogenetic proteins) influence cell condensations and cause chondrogenesis and osteogenesis. BMPs are members of the transforming growth factor-β superfamily. The more than 20 BMP-related proteins which have been identified can be classified into subgroups depending on their structure and function. They play important roles in determining the fate of mesenchymal cells by stimulating their differentiation into osteoblastic cells and by inhibiting their differentiation into myoblastic cells. They increase osteoclastogenesis which is coordinated with osteoblastogenesis through coupling factors.
When BMPs have bound to and activated their receptors they cause cell signalling by phosphorylating cytoplasmic receptor-regulated Smads (R-Smads, Sma 1, 5 and 8). The R-smads which have been activated form heterodimers with the common partner Smad (Co-Smad, Smad4) and after having reached the nucleus of the cell they attract distinct transcription cofactors and regulate transcription.
Similarities in their amino-acid sequences can be used to divide the BMPs into three subgroups: The first group is the BMP2/4 group including BMP2 and BMP4, and the Drosophila decapentaplegic (dpp) gene product. The second group consists of the osteogenic protein 1 (OP1) group which includes BMP5, BMP6, OP1 (BMP7), BMP8 (OP2) and the Drosophila gbb-60A gene product. The third group consists of the growth-differentiating factor 5 (GDF5) group which includes GDF5, GDF6 (BMP13), and GDF7 (BP12). BMPs have distinct spatiotemporal expression patterns and they bind to their receptors with different affinities and in combinations which causes the biological activities to be different. BMP1 is not related to other BMPs and it does not regulate the growth and differentiation of skeletal cells. BMP1 is a protease which cleaves procollagen fibrils and also chordin. Chordin can inhibit the actions of BMP2/4 by binding to them.
BMPs bind to different sets of receptor complexes which determine the type of intracellular signals. There are three type 2 receptors for BMP signalling: BMP type 2 receptor (BMPR2); activin type 2A receptor (ActR2A); and activin type 2B receptors (ActR2B). The three type 1 receptors are activin receptor-like kinase (ALK)2; ALK3 (BMPRIA); and ALK6 (BMPRIB). BMP2 and BMP4, which have potent osteogenic effects, have affinity for ALK3 and ALK4. Members of the OP1 group bind to ALK2 and ALK6. BMPs of the GDF group bind to ALK6 but not to other receptors. Mullerian inhibiting substance (MIS) (= anti-Mullerian hormone (AMH)) which is a member of the TGF-β superfamily binds to the unique receptor complex consisting of the BMP type 1 receptor and AMH type 2 receptor to cause BMP-like signalling. Even before BMPs have attached to them type 1 and type 2 BMP receptors on the cell surface exist as either homomeric or heteromeric complexes. Attachment of BMP2 rearranges receptor complexes at the cell surface. When BMP2 binds to a receptor complex which is already heteromeric this binding causes the activation of the smad pathway but when BMP2 binds to a receptor complex and causes it to be heteromeric a Smad-independent pathway is activated with the result that alkaline phosphatase is activated through p38 MAP kinase. It is believed that the specific structure of the BMP receptors before BMP binds to them determines which signalling pathway will be activated.
The proteins PKCβ, tubulin β5 and MAPKKK8, which are involved in skeletal development including migration, differentiation and apoptosis, interact with the C-terminal domain of BMPR2. This means that this receptor has unique signalling properties.
When cells in a condensation start to differentiate it necessitates the downregulation of genes which control proliferation and the upregulation of genes responsible for differentiation through pathways exemplified by BMP2, BMP4 and BMP5. The transition from proliferating chondroblasts to chondrocytes and hypertrophic chondrocytes is regulated by BMP via Indian hedgehog (Ihh). Ihh promotes chondrogenesis and enchondral ossification. BMPs cause maturation when they act directly on chondrocytes and this effect is counterbalanced by initiation of the Ihh/PTHrP signalling loop.
Id genes are BMP-dependent, dominant negative regulators of helix-loop-helix transcription factors and influence cell growth and differentiation. To achieve terminal differentiation in bone morphogenesis it is necessary to downregulate Id genes. BMPs upregulate Id proteins in mesenchymal cells which prevents them from differentiating into myoblasts and adipocytes. Normal skeletal development in developing limbs necessitates apoptosis, which is induced by BMPs.
The differentiation of stromal cells to osteoblasts is caused by BMP2 and this effect is counteracted by TGF-β. BMPs cause increase of IGF-1 (IGF = insulin-like growth factor) and IGF-2 mRNA. IGF-1 and IGF-2 improve osteoblastic function. p38, a MAP kinase (MAP = mitogen activated protein) and ERK (= extracellular receptor kinase) is necessary when BMP2 induces higher levels of type 1 collagen, fibronectin, osteopontin, osteocalcin and alkaline phosphatase activity.
Nephroblastoma Overexpressed (Nov). Nov is a member of the CCN family of proteins. Nov was identified in avian nephroblastoma caused by myeloblastosis-associated virus. It is expressed by osteoblasts and its transcription is regulated by transforming growth factor (TGF)-β and bone morphogenetic proteins (BMPs). CCN proteins can interact with TGF-β, BMPs and Wnt. Nov has an antagonistic action against BMP and inhibits osteoblastogenesis and the function of osteoblasts.
Extracellular BMP antagonists, which may be synthetized by osteoblasts, can obstruct BMPs from binding to cell surface receptors and in that way prevent BMP signalling. BMP antagonists often diminish the action of Wnt, which is a signal regulating osteoblastogenesis. Wnt activity, as well as BMP activity, is controlled by extracellular and intracellular antagonists.
The CCN family of cysteine-rich (CR) secreted proteins encompasses cysteine-rich 61 (Cyr 61), connective tissue growth factor (CTGF), nephroblastoma overexpressed (Nov) and Wnt-inducible secreted proteins (WISP) 1,2 and 3. Cyr 61 and CTGF have an effect on cell adhesion, angiogenesis, chondrogenesis and on the development of the embryonic skeleton. WISP 1 augments the effect of BMP on osteogenesis. Nov is also expressed in hypertrophic cartilage and it has angiogenic properties and it enhances TGF-β2 signalling in chondrocytes but not in osteoblasts. Nov interacts with Connexin 43 which is a molecule important for cell-cell communication, skeletal development and osteoblast function.
PTHrP. PTHrP (= parathyroid hormone related peptide) gene-expression products are to be found in the periosteum and in insertions sites of ligaments and tendons. The Indian hedgehog-PTHrP axis is located in the articular cartilage, where it is believed that it prevents the joint space from invasion of mineralizing cells, and in the growth cartilage postnatally. Generally, there is a mechanical regulation of PTHrP in these locations.
Axin1 and axin2. Chondrocyte maturation is slowed by signalling by transforming growth factor-β (TGF-β)/Smad3 and it is enhanced by signalling by Wingless/INT-1 related (Wnt)/β-catenin. The two functionally equivalent isoforms Axin1 and Axin2 inhibit Wnt/β-catenin signalling and enhance TGF-β signalling ("crosstalk between signalling pathways"). Wnt3a stimulates Axin2 in a negative feedback loop and TGF-β inhibits the expression of both Axin1 and Axin2 and enhances β-catenin signalling. Axin1 and Axin2 integrate signals between the Wnt/β-catenin and TGF-β/Smad pathways. Because the inhibition of the expression of Axin1 and Axin2 caused by TGF-β will inhibit TGF-β signalling and will augment the Wnt/β-catenin signalling the end effect is a change from TGF-β to Wnt/β-catenin signalling which will enhance maturation of chondrocytes.
TGF-β and PTHrP slow the rate of maturation of chondrocytes while BMPs, thyroid hormone, retinoic acid and Wingless/INT-1-related (Wnt) proteins augment the rate of maturation of chondrocytes.
Schnurri-3. Schnurri-3 (Shn3), a zinc finger adaptor protein, has been reported to regulate bone mass. Mice lacking Schnurri-3 have increased bone mass. Shn3 attracts WWP1, a Nedd4 family E3 ubiquitin ligase, to the important transcriptional regulator of the osteoblast, Runx2. WWP1 normally degrades Runx2 so when there is a lack of Shn3 the degradation of Runx2 is diminished which leads to an increased concentration of Runx2 resulting in the increased expression of Runx2 target genes and increased osteoblast production of bone. WWP1 is able to polyubiquitinate Runx2 and to accomplish a proteasome-dependent degradation of Runx2.
With the aid of nuclear transcription factors, coactivators and adaptor proteins the transcription factor Runx2 interprets extracellular signals in order to regulate osteoblast differentiation. Runx2-/- mice do not have any intramembranous or enchondral ossification. Runx2 has a central function regarding osteoblast differentiation during embryonic differentiation. Runx2 also controls the activity of osteoblasts in adult mice through induction of the transcription factor ATF4 which regulates collagen synthesis in mature osteoblasts. The interaction of Shn3 with TRAF2 inhibits responses which have been created by NF-κB and JNK such as apoptosis and expression of the TNF-α gene.
PPAR. PPAR (peroxisome proliferator-activated receptor-γ (PPAR-γ) participates in two signalling pathways which change the fate of common pleiotropic mesenchymal cells to osteoblasts instead of being transformed to adipocytes. One of these signalling pathways is the TAK1/TAB1/NIK cascade which is activated by TNF-α and IL-1. This pathway activates NF-κB to prevent PPAR from binding to the DNA which diminishes the creation of adipocytes. The other signalling pathway is the noncanonical Wnt pathway comprising CaMKII-TAK1/TAB2-NLK. Wnt-5a, a noncanonical Wnt ligand, under the influence of activated NLK inhibits PPAR transactivation by the use of SETDB1 which is a histone methyltransferase. Wnt-5a causes phosphorylation of NLK and a corepressor complex is formed which inactivates the function of PPAR by methylation of histone H3-K9.
The formation of osteoblasts is influenced by several cytokines and Wnt peptide ligands. Through the binding to frizzled (Fzd) plasma membrane receptors by several Wnt ligands canonical and noncanonical Wnt signalling pathways are activated. The activation of the canonical pathway implies stabilization and transfer to the cell nucleus of the intracellular transducer β-catenin where contact is established with members of the T-cell factor/lymphoid enhancer factor (TCG/LEF) family of transcriptional factors for the activation of the transcription. PPAR-γ is a member of the NR gene superfamily that are ligand-inducible transcription factors controlling the expression of target genes by remodelling of chromatin and modifications of histone. Special combinations of histone modifications constitute a "histone code" and is used for transcriptional control.
Transcriptional regulation of osteoblasts. The transformation of mesenchymal precursor cells to osteoblasts is achieved by a series of transcription factors, for example Runx2, Osterix (OSX), ATF4 and nuclear coregulators. Runx2 is of importance at several stages in bone formation and is regulated by nuclear accessory factors and posttranslational modification, above all phosphorylation. Interactions with DLX proteins and ATF4 and phosphorylation by the ERK/MAP kinase pathways are examples of regulation of Runx2. The phosphorylation of Runx2 takes place at serine residues in the P/S/T domain. Bone formation is influenced by ECM (= ExtraCellular Matrix), mechanical loads where integrins are mediators, and hormones.
Runx2 is necessary for the development of bone and hypertrophic cartilage and already is present during the formation of mesenchymal condensations which later are transformed to bone and cartilage. Other different transcription factors cooperate with Runx2 to transform mesenchymal precursor cells to chondrocytes and osteoblasts. Osterix (Osx) makes osteochondroprogenitor cells transform to osteoblasts. The transcription factor ATF4 controls the transcriptional activity of mature osteoblasts. Runx2 also is necessary for the transformation of osteochondroprogenitor cells to chondrocytes. At the beginning it is suppressed by the chondrocyte-specific factors Sox8/9. In order to promote chondrocyte hypertrophy the Sox factors are downregulated.
FIAT. FIAT (Factor Inhibiting ATF4-mediated Transcription) is a leucin zipper protein which interacts with ATF4 and prevents it from transcribing the osteocalcin gene. FIAT is a protein located in the nucleus but does not bind to the DNA. It has three leucine zipper domains, one of which is used to heterodimerize with ATF4 preventing it from binding to the DNA. FIAT also blocks the transcriptional activity by a c-Jun--Fra-1 heterodimer. This means that FIAT can influence early activity of the osteoblast by interaction with ATF4 as well as later activity of the osteoblast by interaction with Fra-1.
When ATF4 is activated by the ribosomal S6 kinase 2 (RSK2) it regulates the start of the differentiation of the osteoblast, and the transcription of osteocalcin and collagen 1. When ATF4 is activated by protein kinase A (PKA) phosphorylation it starts the transcription of the RANKL gene and thus influences the formation of osteoclasts. Ectopic expression of Fra-1 results in the increase of bone mass caused by an increase in osteoblast differentiation. The inactivation of Fra-1 results in osteopenia.
Calcineurin Aα. Calcineurin (CN) is sensitive to calcium and calmodulin and is a serine to threonine phosphatase. It is a heterodimer with catalytic and regular subunits and α, β and γ isoforms which all are expressed on osteoblasts and osteoclasts. Deletion of the gene coding for the isoform calcineurin Aα (CNAα) causes osteoporosis due to impaired production of bone. Forced expression of CN increases markers of osteoblastic differentiation and bone formation. CN is beneficial to osteoclastogenesis and it impairs the resorption of bone.
When CN dephosphorylates the transcriptional regulator NFAT2, which is downstream of CN and is of importance to both osteoblasts and osteoclasts, it causes NFAT2 to localize in the nucleus and to bind with API transcription factors to gene promotors in the precursor of the osteoclast, and to bind with osterix to gene promotors in the precursor of the osteoblast.
NFAT and the osteoclast. Together with M-CSF (macrophage-colony-stimulating factor) and costimulatory signals, RANKL (receptor activator of NF-κB ligand), which is a TNF superfamily cytokine, causes formation of osteoclasts (inhibition of the interaction between RANKL and RANK, RANK is the receptor for RANKL, through the administration of osteoprotegerin which binds to RANKL, i.e. osteoprotegerin functions as a decoy receptor and prevents it from binding to RANK, decreased bone resorption and joint deformation in experimental LCPD in piglets (20)). RANKL activates the TNF receptor-associated factor 6 (TRAF6) and the cFos pathways. This results in an event specific for osteoclasts, the autoamplification of nuclear factor of activated T-cells (NFAT)c1. The autoamplification of NFATc1 depends on the signalling of calcium of immunoglobulin-like receptors which are associated with adaptors having an immunoreceptor tyrosin-based activation motif (ITAM). Calcium activates the calcineurin-NFATc1 pathway and also the calmodulin-dependent kinase pathway, both are important for the formation of osteoclasts.
RANK, the receptor for RANKL, is expressed in the precursor cells of the osteoclast and also in mature osteoclasts. Osteoprotegerin (OPG) is an inhibitor of RANKL because it binds to RANKL and prevents it from binding to its natural receptor RANK ("soluble decoy receptor"). The intensity of bone resorption is determined by the balance between OPG and RANKL. It is believed that the TRAF6-NF-κB and c-Fos pathways are downstream signalling events which are activated by RANKL. TRAF family proteins are adaptor molecules for various cytokine receptors including the TNF receptor superfamily and members of the Toll/IL-1 receptor family. RANK has three binding sites for TRAF6 .
The transcription factor which is most strongly induced by RANKL is NFATc1. The NFAT transcription factor family comprises five members: NFATc1 (NfAT2), NFATc2 (NFAT1), NFATc3 (NfAT4), NFATc4 (NFAT3) and NFAT5. Calcium/calmodulin signalling activates a specific phosphatase, calcineurin, which activates NFAT.
NFAT1c regulates osteoclast-specific genes and has a gene regulatory mechanism involving autoamplification where NFAT1c is attracted to its own promotor.
Bim and Caspase-3 in apoptosis. Bim is a proapoptotic BH3-domain-only member of the Bcl-2 family the expression of which is regulated at the transcriptional and the posttranslational level, the latter involving phosphorylation and ubiquitination. It is believed that caspase-3 causes Bim to be degraded, i.e. that there is a negative feedback loop in the axis of Bim-caspase.
The genetically programmed cell death to eliminate unwanted cells is called apoptosis. The two kinds of apoptosis are the death receptor pathway and the mitochondrial pathway. Bim uses the pathway of mitochondrial apoptosis through the release of cytochrome c from the mitochondria. The cytochrome c which has been released interacts with Apaf-1 and caspase-9 to create the apoptosome in which caspase-9 activates effector caspases, caspase-3 and caspase-7, which leads to apoptosis. It has been shown that Bim is necessary for the apoptosis of T-lymphocytes, B-lymphocytes, myeloid cells, neurons and osteoclasts.
TRAIL and apoptosis. TRAIL ( TNF-related apoptosis-inducing ligand) belongs to the TNF superfamily and causes apoptosis of neoplastic and normal cells. DR5, a death receptor, is upregulated by TRAIL and is regarded to be the mediator of apoptosis in osteoclasts caused by TRAIL. Earlier it has been shown that apoptosis of osteoclasts also is caused by the Fas/FasL system.
Glucocorticoids. Glucocorticoid (GC) causes loss of bone and is a common cause of osteoporosis. Dexamethasone inhibits M-CSF in its activation of RhoA, Rac and Vav3, these three factors regulate the cytoskeleton of the osteoclast, the cytoskeleton includes the actin ring which is in direct contact with bone and separates the resorptive environment from the extracellular environment. Dexamethasone impairs the activity of osteoblasts through the influence of osteoclasts. GCs have direct and indirect effects on the skeleton. Indirect effects include impaired release of sex hormones and impaired absorption of calcium in the kidneys and the intestinum.
Vitamin D. Calbindin, a protein which binds calcium, has an important function in the protection against apoptotic cell death in various tissues including protection against cytokine-mediated apoptosis in osteoblasts. The two major subclasses of calbindin are calbindin-D9k and calbindin-D28k, the latter exists in, among other cell types, osteoblastic cells. Calbindin-D28k prevents apoptosis by the buffering of calcium, a prolonged high intracellular concentration of calcium causes cell death. Inhibition of caspase 3 also is a mechanism of the antiapoptotic effect of calbindin-D28k, this mechanism is not dependent on the ability of calbindin-D28k to buffer calcium.
The regulation of gene expression in target cells by 1,25(OH)2D3 is accomplished by its binding to the vitamin D receptor (VDR). This binding causes VDR to heterodimerize with the retinoid X receptor (RXR) and this complex binds to vitamin D response elements (vDREs) in the promotor of target genes. Coactivators are recruited and the effect on target gene transcription begins.
In an investigation an Affymetrix gene chip array was used to find targets of 1,25(OH)2D3. One of these identified genes was C/EBPβ which is a nuclear coupling factor coordinating the effects of vitamin D and PTH on the regulation of osteopontin (OPN), a protein having an influence on resorption and mineralization. Both 1,25(OH)2D3 and PTH can activate C/EBPβ in osteoblastic cells. PTH and/or activation of PKA has the ability to increase the induction of the expression of OPN caused by 1,25(OH)2D3.
Parathyroid hormone (PTH). PTH binds to PTH/PTH-related protein 1 receptor on osteoblasts (the text says osteoblasts, not osteoclasts) and the effects are an increase of the blood concentration of calcium and an increase of the expression of matrix metalloproteinase-13 (MMP-13) which degrades components of extracellular matrix. Necessary for this to occur is the binding of Runx2 to the runt domain (RD)-binding site and the binding of activator protein-1 (AP-1) to the AP-1 site. PTH regulates HDACs (histone deacetylases) which are of importance in relation to the activity of MMP-13.
Continuous administration of PTH results in elevated calcium in the blood and a reduced volume of trabecular bone. Intermittent administration of PTH on a daily basis results in increased volume of trabecular bone. The Wnt proteins are rich in cysteine and disulphide-linked glycoproteins. When they are secreted the N-terminal signal peptide is removed and they are further glycosylated. A palmitate group is added via a thioester bond on the first cysteine (C77).
The two functional classes of Wnts are Wnt-1 and Wnt-5a. The Wnt-1 class works in the canonical Wnt pathway and the Wnt-5a class has its effect in the noncanonical Wnt pathway. The canonical pathway implies accumulation in the nucleus of β-catenin and activation of transcription targets downstream, for instance Lef/Tcf. This pathway which is believed to be especially active in the osteoblast where it influences cell proliferation and cell-fate determination is called the Wnt β-catenin pathway. The Wnt-5a class uses the noncanonical Wnt pathway which is formed by two signalling pathways. The first of these two pathways is the PKC pathway (Wnt/Ca2+) via cGMP proteins, via activation of phospholipase C and phosphodiesterase which increases the concentration of calcium ions intracellularly. The second pathway of the noncanonical Wnt pathway is Wnt/PCP (planar cell polarity pathway) which influences organization of the cytoskeleton via JNK which is a member of the MAP kinases.
In the developing chick limb, the noncanonical Wnt-4 and Wnt-5a and Wnt-5b are expressed in chondrogenic areas. Wnt-5b is expressed in prehypertrophic chondrocytes and Wnt-4 is expressed in the joint regions. Overexpression of Wnt-4 causes the chondrocyte differentiation and the creation of a bone collar to accelerate which might signify that Wnt-4 influences the differentiation of the osteoblast in the periosteum. It is believed that there is cross-talk between the canonical and noncanonical Wnt pathways depending on the maturity and differentiated state of the cell. PTH stimulation of Wnt-4 is mostly via the PKA pathway.
T cells. There is reason to believe that oestrogen prevents the loss of bone through its influence on T-lymphocytes (T-cells) which influence the formation, life span and activity of osteoclasts. The increased resorption of bone due to the deficiency of oestrogen is to the largest part caused by the increased formation of osteoclasts because of cytokines, for instance TNF produced by T-cells and this through a complicated pathway involving several cytokines and immune cells. Through costimulation via CD40 to CD40 Ligand (CD40L) T-cells have an influence on the production of osteoprotegerin (OPG) manufactured by B-cells. The earlier assumption that the osteoblast or its immediate precursor, the bone marrow stromal cell, was the dominant producer of OPG has now been replaced by the assumption that the B-cell is the dominant producer of OPG in bone. T-cells can produce cytokines which are osteoclastogenic such as RANKL, TNF and also cytokines which are anti-osteoclastogenic, for instance IL-4 and IFN-γ .
FSH. FSH (follicle-stimulating hormone) presumably enhances bone resorption by osteoclasts. In vitro it has been shown that oestrogen has a weak and direct inhibitory effect on precursors of osteoclasts through the interference with phosphorylation of the janus N-terminal kinase which is downstream of receptor activator for NF-κ B-ligand (RANK-L). With the use of several pathways oestrogen also influences the secretion of the osteoclastogenic cytokine (RANK-L) and its decoy receptor osteoprotegerin (OPG) from osteoblasts. The effect on osteoclastogenesis exerted by oestrogen is also mediated via T-cells, through production of TNF-α.
FSH enhances the formation of osteoclasts from bone marrow precursors in the presence of RANK-L. FSH has a osteoclastogenic and proresorptive effect which is mediated by a Gi2α receptor present in osteoclasts and precursors of osteoclasts. FSH increases the phosphorylation of downstream kinases, Erk and Akt, which are sensitive to RANK-L, and Ik-Bα, an inhibitor of NF-κB. These pathways effectuate the proresorptive effects of RANK-L.
TSH and thyroid hormone. In thyrotoxicosis there is an elevated concentration of thyroid hormone which leads to a lower concentration of TSH (thyroid stimulating hormone = thyrotropin), a consequence is an increase of the turnover of bone and a diminished bone mass. Both thyroid receptors (TRs) and TSH receptors (TSHRs) influence the remodelling of bone.
Through nuclear TRs α and β thyroid hormones increase the resorptive function by osteoclasts via osteoblasts. Cytokines and hormones which have a function in the activation of osteoclasts include IL-6, PGE2, PTH and vitamin D. TRα is more abundant that TRβ in bone and is believed to be of greater importance. Analysis of TR knockouts (genetically manipulated mice where a gene has been made unfunctional) reveals a difference in function between the two isoforms of the TR receptor concerning their effects on bone. It is not known whether the phenotype of adult bone in these knockouts is caused by defects in maturation or is an effect on the adult bone and the cellular and molecular events responsible for the maturation of bone are not known either.
Thyroid hormones have an influence on the differentiation of chondrocytes by determining the set-point of the Ihh-BMP-PTHrP long feedback loop (Ihh = Indian hedgehog, BMP = bone morphogenic protein, PTHrP = parathyroid hormone-related protein). Thyroid hormones also regulate the checkpoint of G1-S cell cycle through the induction of cyclin-dependent kinase inhibitors. Thyroid hormones also elevate the activity of alkaline phosphatase and the proangiogenic factor collagenase 3.
Thyroid hormones are essential for morphogenesis and growth of bone but to much of them, hyperthyroidism, leads to an elevated bone resorption. Subclinical hyperthyroidism, normal levels of thyroid hormone and low level of TSH, leads to increased resorption of bone and loss of bone. TSH can diminish both the formation of bone and the resorption of bone. It is suggested that TSHRs have effects on the remodelling of bone that are independent of the levels of thyroid hormones.
TSH has an influence on the function and formation of osteoclasts and osteoblasts, it impairs the differentiation of osteoblasts and the synthesis of collagen. TSH has a negative effect on the formation of osteoclasts caused by RANKL through an effect on two signal transduction steps which involve inhibitor IkBα and JNK. These events cause lower levels of the proosteoclastogenic transcription factors c-jun and p65. The lower level of c-jun diminishes the transcription of the tartrate-resistant acidic phosphatase (TRAP) and cathepsin K genes, which are necessary to the resorptive action of osteoclasts. The downstream effects of TSH are mediated by the cytokine TNF-α.
G-CSF and SNS. G-CSF (granulocyte colony - stimulating factor) is used in the clinic to mobilize HSPCs (hematopoietic stem and progenitor cells) from the bone marrow to the systemic circulation and this factor impairs the function of osteoblasts. The osteoblast does not have a receptor for G-CSF and it is believed that the impairment of the osteoblast caused by G-CSF is an indirect effect and that signals from SNS (sympathetic nervous system) are required for this impairment.
That SNS has an influence on the proliferation and function of osteoblasts and on the formation of bone is indicated by several clinical and experimental findings. Through signals from SNS with an origin in the ventromedial hypothalamic nucleus the hormone leptin can decrease bone mass. SNS can enhance the resorption of bone by enhancement of the differentiation of osteoclasts. It is also suggested that SNS has an influence on the proliferation of osteoblasts via the core genes of the molecular clock Per 1 and Cry which indicates that circadian regulation is active here. In the endosteum nerve fibers containing catecholamine, glutamate and vasoactive intestinal peptide are in close proximity to osteoblasts and osteoclasts.
Endocannabinoid System. The endocannabinoid system with the CB1 receptors in nerve terminals of the SNS (sympathetic nervous system) in bone and the CB2 receptors in osteoblasts and osteoclasts has an influence on bone. In bone CB2 has a greater influence than CB1. In experimentally caused loss of bone, activation of CB2 diminishes the bone loss through an inhibition of the resorption of bone and the enhancement of the formation of bone.
The differentiation of osteoclasts is under the influence of RANKL (receptor activator of NF-κB ligand), osteoprotegerin (OPG), macrophage colony-stimulating factor (M-CSF) and interleukin 6 (IL-6). Stromal cells in the vicinity including osteoblasts and precursors of osteoblasts provide these factors. The formation of bone is under the influence of BMPs, parathyroid hormone (PTH), calcitonin, insulin-like growth factor 1 (IGF-1) and the osteogenic growth peptide (OGP). The remodelling of bone is also under the influence of a central control through the signalling of hypothalamic leptin and neuropeptide Y as well as by norepinephrine (NE) signalling via β2 adrenergic receptors in osteoblasts.
Both CB1 and CB2 receptors are generally coupled directly to the G(i/o) subclass of G proteins and they cause the inhibition of stimulated total activity of adenyly1 cyclase. In contrast, CB activation may increase the activity of several subtypes of adenyly1 cyclase, presumably the type of cell and cannabinoid ligands are of importance. The cannabinoid receptors also cause the activation of p42/p44 mitogen-activated protein kinase (MAPK), c-Jun N-terminal kinase, AP-1, the neural form of focal adhesion kinase, protein kinase B and Ca2+ transients.
The main endogenous ligands of CB1 and CB2 are N-arachidonoylethanolamine (AEA or anandamide) and 2-arachidonoylglycerol (2-AG). Anandamide is believed to be a partial agonist to CB1, and AG-2 is assumed to be a full agonist of both CB1 and CB2 receptors. Leptin exerts a negative regulation of 2-AG. Traumatic head injury activates the formation of bone and central production of 2-AG.
In cultures of osteoblastic cells the expression of CB2 mRNA is elevated as the expression of marker genes for the osteoblasts such as tissue nonspecific alkaline phosphatase (TNSALP), parathyroid receptor 1 (PTHRc1) and RUNX2 increases. In monocytic cells which are being transformed to osteoclasts CB1 expression is low but the expression of CB2 is high. CB2 has different effects on the formation and function of osteoblasts depending on the level of differentiation and it also has a negative effect on osteoclastogenesis. Through binding to β2-adrenergic receptors on osteoblasts NE (norepinephrine) impairs the function of osteoblasts. There is evidence that activation of sympathetic CB1 lessens this effect of NE. The cannabinoid psychoactivity is caused by CB1 and not by CB2.
Androgens. Androgen receptors (AR) exist in osteoblasts, osteoclasts and stromal cells of the bone marrow. In a cell culture DHT (dihydrotestosterone) enhances the differentiation of the preosteoblasts along with an elevated canonical Wnt signalling. The pathway of canonical Wnt signalling is an important pathway as regards the commitment of the bone mesenchymal cell lineage and enhances the differentiation of osteoblasts and the production of bone. As a consequence of an increased canonical Wnt signalling there will be an increased expression of target genes which lead to enhanced phosphorylation of GSK3β and an increased level of nuclear β-catenin and Runx2. This effect on the differentiation of preosteoblasts is inhibited by soluble frizzed-related protein (sFRP) which is a Wnt antagonist occurring naturally.
Tumor Necrosis Factor (TNF) Family Receptors. The TNF receptors are of importance in the differentiation and activity of both osteoblasts and osteoclasts but the exact mechanism is in several cases not completely known. RANKL and TNFα are key regulators of the formation of osteoclasts. TNF receptors (TNF-R) in osteoblasts and in precursors of osteoblasts include TNFR1 (p55), DR3 (TNFR25) (alternatively spliced to produce cell membrane forms and soluble receptors), DR5 (TRAIL-R2) and FAS and perhaps also FN14 and DR4 (TRAIL-R1). Apart from having cell membrane TNF receptors osteoblasts produce soluble TNF-receptors such as DcR2, osteoprotegerin and sDR3. These soluble receptors bind the TNFs TRAIL, RANKL, TL1A and Apo3 and block the effects of ligands on cell surface receptors. The activation of D3 has an influence on the maturation of osteoblasts and may make preosteoblasts unable to differentiate. TL1A is a major natural ligand for DR3 which is produced by vascular cells in the vicinity of differentiating osteoblasts and perhaps also by precursors of osteoclasts which have been stimulated by Fcγ. The soluble DR3 splice variant produced by osteoblasts regulates the activity of DR3.
TNF-Rs (TNF receptors) exist in groups with 3-5 extracellular cysteine-rich globular domains that interact with ligand(s). The intracellular part of the receptors includes common domains that are linked to specific pathways of differentiation and cell death. Several of the receptors have TRAF-activating (differentiation) domains which are coupled to other pathways including jun-kinase activation.
The parallel activation of common intracellular pathways by several receptors and also the fact that several kinds of ligands may bind to a receptor ("ligand degeneracy") complicates TNF receptor signalling. An example of ligand degeneracy is the soluble TNF-R family decoy receptor osteoprotegerin which can bind both TRAIL and RANK.
Comparison with NEE. The articles summarized above are based on investigations that have had the objective to clarify the mechanism responsible for regulating the homeostasis of bone. They do not have had the purpose to clarify mechanisms which would be of use for the four motifs in NEE. An increased production of bone, eventually leading to osteopetrosis, is not equivalent to an increase of the macroscopic volume of bone which is needed for an advancing motif, i.e. to eliminate a deficit volume and a net decrease of bone density leading to osteoporosis is not equivalent to decreasing the macroscopic volume of bone which is needed for a retreating motif, i.e. to eliminate redundant volume.
Motif number one implies the elimination of deficit volume where the deficit volume is bounded by the articular cartilage. Skeletal Biology and Medicine, Part A does not provide any information concerning why the superficial cells in the articular cartilage ("stem cells") stop to divide in adolescence. It does not provide any information concerning the possible difference in the genetic setup between an actively dividing stem cell and a stem cell which has ceased to divide in adolescence and it does not comment upon what would be needed from a gene therapy to eliminate that difference. It does not comment upon how many mitoses (more than one or not) there are in the vertical direction, from the surface of the articular cartilage down to the hypertrophic zone of the articular cartilage and it does not comment upon what would be required from a gene therapy to introduce one or two or possibly three more mitoses in the vertical direction with the purpose to increase the growth velocity of the articular cartilage and it does not describe how this increased growth velocity of the articular cartilage could be started and stopped at will which would be needed by NEE.
An advancing motif does imply recruitment of and synthetic activity by osteoblasts and a retreating motif does imply recruitment of and resorptive activity by osteoclasts. Preliminarily we may put in the basket of advancing motifs BMP2 and BMP4 and in the basket of retreating motifs we may put RANKL.
A quick reading of the 2006 revision of the nosology and classification of genetic skeletal disorders with its 372 disorders in 37 groups (21) (to see if nature's own experiments provide candidates for relevant growth factors for the different motifs) identifies familial expansile osteolysis as a rare autosomal dominant bone disorder where osteolytic lesions show increased osteoblast and osteoclast activity because of a mutation in the receptor activator of nuclear factor-κB (RANK) (22).
Femoral head epiphysis growth has been studied in Chinese children (23). At the age of twelve months the right and left femoral head epiphysis had a diameter of 10.45 mm and 10.45 mm for boys and 10.23 mm and 10.68 mm for girls. At the age of 19-24 months the right and left epiphysis had a diameter of 14.25 mm and 14.35 mm for boys and 14.42 mm and 14.20 mm for girls. The increase in diameter for the right and left femoral head epiphyses was 14.52 mm - 10.45 mm = 4.07 mm and 14.35 mm - 10.45 mm = 3.90 mm for boys and 14.42 mm - 10.68 mm = 3.74 mm and 14.20 mm - 10.23 mm = 3.97 mm for girls. The average increase in the diameter of right and left femoral head epiphysis was (4.07 mm + 3.90 mm + 3.74 mm + 3.97 mm)/4 = 3.92 mm. Half of the value corresponds to the increase of the radius of the femoral head epiphysis, 3.92 mm/2 = 1.96 mm. This increase in the radius was achieved in 7-12 months. If this time period is averaged to (7+12)/2 = 9.5 months the average velocity in increase of the radius of the femoral head epiphysis is 1.96 mm/9.5 months = 0.21 mm/month = 2.48 mm/year. (Calcification of the epiphyses was often not seen at the age < 12 months, one has to differentiate between the rate of calcification of already existing cartilage and increase in diameter of the epiphysis). With this growth velocity in the articular cartilage to bridge a 40 mm deficit volume the time needed would be 40 mm/ 2.48 mm per year = 16 years.
This relatively low growth rate can be compared with the growth rate of the articular cartilage of the high-weight-bearing areas of the femoral condyles of the New Zealand white rabbit which is at its maximum at the age of 1 month and amounts to 85-95 μm/day (24). If this growth rate could be achieved in the articular cartilage for motif no. 1 to eliminate a 40 mm long deficit volume it would take 40 mm/((((85+95)/2) x 0,001 mm)/day) = 444 days = 1 year and 3 months which is a more suitable growth velocity.
One could imagine that the epiphysis grows by two different mechanisms. The first mechanism would be that growth occurs through the stem cells in the superficial layer of the articular cartilage, appositional growth, and that the basal layer of the articular cartilage is calcified and resorbed and converted to bone tissue allowing the radius of the bone epiphysis to increase.
The other principle would be that growth does not occur in the articular cartilage but only in the bone underlying the articular cartilage and that the articular cartilage shows internal remodelling to adapt to the increased radius of the bone epiphysis.
These are different mechanisms. Hunziker, et al (24) has showed which of these two mechanisms is correct in the New Zealand white rabbit. It is the first mechanism which is correct. Growth occurs in the articular cartilage through division of the stem cells in the superficial portion of the articular cartilage. These stem cells have a bidirectional mitotic activity. Mitotic activity in the horizontal direction causes lateral expansion of the articular cartilage and mitotic activity in the vertical direction gives rise to rapidly dividing daughter cells which cause growth in the vertical direction and would have increased the thickness of the articular cartilage had it not been for the resorption of its basal layer and its conversion to bone. If the conversion of the basal layer of the articular cartilage to bone is inhibited because of an ischemia in the underlying bone and the growth continues in the superficial part of the articular cartilage the thickness of the articular cartilage will increase and this is sometimes seen in LCPD (11).
With the synthesis of new articular cartilage occurring in the superficial layer containing transverse layers of collagen fibres, how is this arrangement of the collagen fibres changed to an arcade-like arrangement in the future middle portion of the articular cartilage and how is this arcade-like arrangement of the collagen fibres changed to a vertical arrangement in the future deep portion of the articular cartilage?
Growth in children has been described by Dimeglio (25). At the bone age of 13 years for girls and 15 years for boys (bone age is assessed according to the method of Greulich and Pyle, an X-Ray is taken of the left hand, wrist and fingers and is compared to an atlas of X-Rays where the development of the epiphyses is shown at different ages) lower limb growth decelerates and stops. The maximum growth velocity in the proximal femoral growth plate is about 0.8 cm/year and in the distal femoral growth plate about 1.2 cm/year. If the latter velocity of 1.2 cm/year could be implemented in the articular cartilage of the deformed femoral head caused by LCPD and used to bridge a 40 mm long distance of deficit volume the time needed would be 40 mm/ 1.2 cm per year = 3 years and 4 months. The growth rate in the distal femoral growth plate is about five times larger than the growth rate of the articular cartilage in the femoral head, (12.0 mm/year)/(2,48 mm/year)= 4.8. Diffusion is a slower process than transport in vessels. An epiphyseal growth plate has vessels on both sides of it whereas the articular cartilage has not. The vascular contribution to osteogenesis has been described by Trueta and Morgan (26), a description of the growth plate and its biochemical regulation has been written by Anderson et al (27), cellular aspects of growth rate can be found in Bone and Cartilage (28).
Bone not covered with articular cartilage has a slower growth. For a simple averaged calculation, assume the diameter of the diaphysis at the age of 17 years is 2.0 cm and that this diameter has been achieved during 17 years, growth rate is then (2.0 cm/17 years)/2 = 0.59 mm/year at the surface of a diaphysis.
If the growth rate was as fast as in the tarso metatarsus of Ardea Cinerea (grey heron), 4.23 mm/day (28), the elimination of a 40 mm long deficit volume would take 40/(4.23/2) = 19 days (to be divided by 2 if it is assumed that the growth rate provided in table 31.1 on page 402 in the book referred to is accomplished by two growth plates and the contributions from the articular cartilages are neglected). If the growth rate was as fast as in the distal femoral growth plate of six-week-old New Zealand white rabbits, 700 μm/day (29), the elimination of a 40 mm long deficit volume would take 40/0.7 = 57 days.
With the use of tritiated thymidine autoradiography of the proximal growth plate of the tibia in the first generation of the August and Marshall strains of rat the growth rate in this epiphyseal cartilage was estimated to 125 μm per day (29). If this growth rate could be maintained in the articular cartilage to bridge a 40 mm long deficit volume it would take 40 mm /(0.125 mm/day) = 320 days ≈ 11 months.
A patient who in his/her early twenties had symptoms from the hip joint and who was given the choice of a treatment which slowly diminished the deformation over a couple of decades with a probable outlook of diminishing symptoms with time, if arthrosis is absent, would probably consider the offer, but, nevertheless, a growth velocity of the articular cartilage greater than 2.48 mm/year would be preferable.
It is not a law of nature that the contour of bone tissue cannot be changed in the adult. An osteoid osteoma, a benign bone tumour, often has a cortical thickening producing a wider diaphysis. If the extra volume in three- dimensional space lying outside the normal contour of the diaphysis occupied by the osteoid osteoma is defined as "deficit volume" it is an example of elimination of deficit volume in the adult. An osteoid osteoma consists of a central nidus of vascularized connective tissue with differentiating osteoblasts producing osteoid (newly formed bone which is not yet calcified) and sometimes bone. The nidus is surrounded by hypervascular sclerotic bone. In two cases involvement of chromosome band 22q13 and loss of the distal part of chromosome arm 17q was found (30). Fracture healing of the diaphysis results in the thickening of the cortex, a widening of the diaphysis, preceded by the vascularization of a blood clot and the formation of callus (initial immature bone formed in the repair of a fracture). If the volume in three-dimensional space outside the original bone volume occupied by the newly formed bone is defined as "deficit volume" it is an example of the elimination of deficit volume in the adult.
Growth can continue into adulthood. A case study (31) describes a man who at the age of 28 years was diagnosed with oestrogen resistance because of a disruptive mutation in the oestrogen-receptor gene. X-Ray of his left wrist and hand showed a bone age of 15 years and knee films revealed open epiphyses. At the age of 16 he was approximately 178 cm tall and at the age of 28 he was 204 cm tall. His legs and feet continued to grow slowly after adolescence.
There is not much time between the end of LCPD and the end of growth in puberty, there will always be a need for NEE in the adult patient.
Histology. A description of articular cartilage can be found in Articular Cartilage (16), Collagen (32,33) and articles from scientific journals (34,35,36). Type Ⅱ collagen, consisting of three identical α1(Ⅱ) chains, is the predominant collagen in articular cartilage. Type Ⅵ, Ⅸ and Ⅺ collagen also exist in cartilage as well as type Ⅹ collagen, the latter in the tidemark, calcified cartilage. Type Ⅵ collagen is located in the pericellular matrix at a higher concentration than outside it Type Ⅸ collagen regulates the fiber diameter of type Ⅱ collagen and probably is responsible for the relatively low fiber diameter of type Ⅱ collagen in the pericellular matrix. The turnover of collagen is slow, more than a hundred years.
The region immediately surrounding a chondrocyte is termed the pericellular matrix and has fine collagen fibres (10-15 nm in diameter), high concentration of proteoglycans, hyaluronan and the presence of fibronectin, type Ⅵ and type Ⅸ collagen, link protein, biglycan, decorin and laminin. The chondrocyte together with the pericellular matrix is called a "chondron". The components that assemble into the aggrecan macromolecule remain separate, which might indicate that the pericellular matrix may have a function to assemble the macromolecule. The pericellular matrix is in turn surrounded by the territorial and interterritorial matrices, the latter two together constitute the extracellular matrix. The territorial matrix has a higher concentration of proteoglycans than the surrounding extracellular matrix and has a finer collagen structure. The interterritorial matrix comprises the bulk of articular cartilage and has a higher concentration of keratin sulphate-rich proteoglycans and collagen fibrils of larger diameter (50 nm or greater) (16).
Lamina splendens, a cell-free proteinaceous thin layer, covers the surface of the articular cartilage. The superficial zone of the articular cartilage (the upper 10-20% of the tissue) has small diameter, densely packed collagen fibers parallel to the cartilage surface. Superficial zone cells secret specific proteins, for example SZP (superficial zone protein, also called proteoglycan 4) that is believed to make the tissue better withstand friction and wear, it is located in the synovial fluid and bound as a thin layer to macromolecules in the lamina splendens. The middle zone (40-60% of the tissue) has spherical cells, type Ⅱ collagen, aggregan, CILP (cartilage intermediate layer protein) and the highest content of proteoglycans. The collagen fibers look like arcades and between them are fibers randomly oriented. The deep zone has large fibre collagens forming bundles perpendicular to the articular surface and anchored in the underlying subchondral bone. The cells are slightly elongated and parallel to the collagen fibers, the cell density is low (16).
Chemistry. In collagen every third amino acid is glycine. The three chains of a collagen molecule constitute three left-handed helical chains with about three amino acids per turn. The three chains are curled around each other in a right-handed twist. Interchain hydrogen bonds are formed but not intrachain hydrogen bonds. The dominant cross-link in collagen is of the pyridinoline type.
The macromolecules which fill the space between cells and collagen are proteoglykans and glycoproteins. The largest proteoglycan is aggregan which consists of a protein core to which are covalently attached GAGs (glycosaminoglycans) via the amino acid serine of the core protein . The core protein of the proteoglykan aggrecan consists of 2316 amino acids and has three globular domains, G1, G2 at the amino-terminal and G3 at the carboxy-terminal. G1 has three functional domains, A, B1 and B2. B1 and B2 interact with hyaluronic acid (HA) to which the core protein binds via a link protein. Between G2 and G3 there are regions for binding of the GAGs keratosulphate and chondroitinsulphate. GAGs are polysaccharides which consist of repeating units of six carbon sugars (hexose or hexuronic acid) which is linked to a six-carbon sugar containing nitrogen (hexosamine). Each proteoglycan aggregate consists of a central hyaluronic acid to which are attached about a hundred aggregan molecules. There are enzymes, aggrecanases, which can cleave aggrecan.
The link protein which connects the aggrecan molecule to hyaluronic acid has a similar structure to the G1 region of the core protein of aggrecan. It has A, B1 and B2 domains. The A domain of the link protein interacts with the G1 region of aggrecan and the B regions interact with HA. Both the link protein and aggrecan are members of the hyalectan family.
Hyaluronic acid (HA), also called hyaluronan, is a non-sulphated GAG contrary to keratosulphate and chondroitinsulphate which are sulphated GAGs, a polysaccharide which consists of repeated disaccharide units of glucuronic acid and N-acetylglucosamine and is synthetized at the plasma membrane by the enzyme hyaluronan synthase (HAS). It is exported directly to the extracellular space where it surrounds the chondrocyte.
The large number of carboxyl and sulphate groups of the GAGs bound to the core protein of aggrecan make them repel each other and to fill every space. An increase in pH and also a decrease in salt concentration increase the repulsion between the GAGs because of reduced shielding of negative charges. These effects have been modelled by molecular dynamics (36). An interlocked supramolecular matrix is formed because of the ability of the GAGs to bind to collagen. The proteoglycan binds to collagen via electrostatically interaction (ion bonds) between the negatively charged GAGs and positively charged amino acids of collagen, especially lysine, hydroxylysine and arginine. Divalent cations can enhance the binding between GAGs and collagen.
The high water content in articular cartilage is caused by the hydrophilicity of the GAGs. When the articular cartilage is compressed water flows out of it and when the pressure is relieved water, together with nutrients, flows in again. This is the background for the fact that intermittent compression is necessary for the nutrition of articuar cartilage.
There also exist smaller proteoglycans, small leucine-rich repeat proteoglycans (SLRPs). The most abundant of these are biglycan, fibromodulin, lumican and decorin. They can interact with, form a protecting coat to, the collagen fibrils and in that manner protect the collagen fibril from degradation by collagenases (MMP1 and MMP13). SLRPs can also regulate growth factor access to the chondrocytes.
Glycoproteins, contrary to proteoglycans, have only a minor carbohydrate component and the carbohydrate is in the form of heteropolysaccharides instead of homogenous repeating disaccharide units as in proteoglycans. Examples of ground substance glycoproteins are fibronectin, laminin and chondronectin.
Permeability. There are no vessels in articular cartilage which for its nourishment is dependent on the synovial fluid with intermittent compression and also on the epiphysis. To achieve the first motif, the elimination of deficit volume when the articular cartilage covers the bone tissue bordering on the deficit volume, the conjugates have to reach the cells of the articular cartilage in order to permit the promotors to reach the nucleus of the cells. Within the intercellular matrix of the articular cartilage molecules are transported by diffusion. The articular cartilage is the most important and troublesome tissue in NEE.
Ekholm (37) in a radioautographic study of the knee-joints injected radioactive phosphorous in the form of Na2HPO4 and radioactive gold in the form of H2(AuCl3) intravenously in rabbits weighing 2.0 - 2.5 kg. Two zones of maximal density were found corresponding to the basal and superficial zones of the articular cartilage, the latter zone extended in general 1/5 - 1/4 through the cartilage section. Passive exercise did not increase the depth of this zone. The intermediate zone appeared to show a higher density of blackening in the exercised joint compared to the unexercised joint, the entire section in the exercised joint was denser. Joint exercise increases the fluid content of the cartilage. It was concluded that articular cartilage is nourished from the joint surface and from the epiphysis.
The diffusion of dyes through articular cartilage in vivo has been investigated by Brower et al (38). 10-20 minutes after the intraarticular injection in the knee of 2-3 months old rabbits with the dye neutral red (MW = Molecular Weight = 288.78 g/mole) the chondrocytes completely stained in the articular cartilage. Within twenty minutes after injection of the cationic dyes toluidine blue (MW = 305.83 g/mole) and methylene blue (MW = 319.86 g/mole) the articular cartilage was completely stained whereas the anionic dyes alizarin red S (MW = 342.26 g/mole) and Evan's blue (MW = 960.8 g/mole) did not stain the articular cartilage. To test if a dye injected into the systemic circulation could stain the articular cartilage the dye neutral red was injected into the aorta of immature rabbits. The superficial cells of the articular cartilage were stained, it was supposed that the dye had entered the joint cavity from the synovial membrane. It was concluded that there is minimal nutritional exchange between the epiphyseal bone and articular cartilage at any age.
The largest molecule which can diffuse into the intercellular matrix has the size of about haemoglobin (MW = 68000 Da (Daltons) = 68000 g/mole). The shape (compact/branched) and charge also are of importance (39). The mean hydrodynamic radius of articular cartilage is about 4-5 nm (40). Using the Poiseuille formula for steady-volume rate of flow through a circular cylinder the radius of a pore through which diffusion can take place has been estimated to about 56Å (41).
Integrins. Integrins are plasma membrane receptors consisting of alpha and beta subunits. They are of importance in cell adhesion and in intra- and extracellular signalling in connection with embryogenesis, haemostasis, tissue repair, immune response and metastatic spread of tumour cells (42).
Application to NEE. In the outline of NEE the text says that the conjugates for motif number one were injected intraarticularly, that was on the assumption that this was to be the less difficult way for the conjugates to reach the chondrocytes within the articular cartilage.
What is required from the articular cartilage in motif number one resembles a 3-step staircase with banisters. The first step of the staircase symbolizes the transport of the conjugate through the intercellular matrix of the articular cartilage and the attachment of the promotor to its intended site in the genome. The second step symbolizes the initiation of growth through division of stem cells located superficially in the articular cartilage. The third step symbolizes the increased growth rate compared to the normal growth rate up to puberty. The banisters symbolize that these three steps are to be performed only in a portion of the articular cartilage, i.e. it is a targeted treatment. When the deficit volume in motif number one is eliminated the promotor should leave its site and the growth should cease. Motif number one implies the walking up this 3-step staircase with banisters, standing on top of the third step and when the deficit volume is eliminated to walk down the staircase.
The articular cartilage in Monodelphis (Monodelphis domestica, grey short-tailed opossum) is similar to the epiphyseal growth plate, being renewed at or near the articular surface and being resorbed at the base through enchondral ossification during the establishment of the subchondral bone and, finally, subchondral plate. Such a mechanism of growth, appositional growth, presupposes an articular cartilage progenitor cell, "stem cell" within the articular surface. As for the growth plate animals with longitudinal proliferating stem cell population in their growth plates could potentially grew throughout life as in amphibians, many reptiles and some fish, "indeterminate growth". Animals with a finite number of proliferating cells show "determinate growth" (28). "Growth plate senescence" (43) is thought to be caused by limited capacity of stem cells in the resting zone to replicate themselves with advancing age. Igf2 (Insulin-like growth factor 2) and also FGF, WNT, eicosanoid, p38-MAPK and vitamin D receptor signalling may be involved.
Cultured human fibroblasts have a limited life-span with a limit to the number of mitoses they can undergo, the "Hayflick limit", associated with a number of morphological and functional changes (44).
Telomers, tandem TTAGGG repeats 5-15 kb in humans, are located at the end of linear chromosomes which decrease in length during cell divisions. They are necessary for genomic stability and survival of the cell. Certain cell types such as germ cells and stem cells contain telomerase, an enzyme which can elongate the telomere through the use of reverse transcriptase activity with an RNA template. The telomer loop (T-loop) prevents the ends of the chromosome from being identified as double-strand breaks. Telomers have a "shelterin" complex of proteins, maintaining telomer homeostasis and responsible for molecular signalling. Reintroduction of telomerase in mice devoid of the enzyme reverted premature aging in spleen, intestine and testes. The telomere has been described as a "replicometer", it measures not time but the number of mitoses performed (44).
The "antagonistic pleiotropy theory" assumes that a particular gene may influence several traits of an organism (pleiotropy). p53 is an example of an antagonistic pleiotropy tumour suppressor gene which can induce senescence and apoptosis and lessen the number of viable stem cells and progenitor cells. Inhibition of another antagonistic pleiotropy gene, mTOR, by rapamycin was reported to restore the self-renewal and hematopoietic potential of aged hematopoietic stem cells, HSC (44).
The "epigenetic landscape", for example DNA methylations and histone modifications, may influence stem cells. Stem cells depend on other cells in their vicinity, the "stem cell niche" (44).
Senescence may be of different types: replicative senescence or telomer dependent senescence, oncogene-inducible senescence and stress-induced (premature) senescence caused by different forms of stress, for example radiation (44).


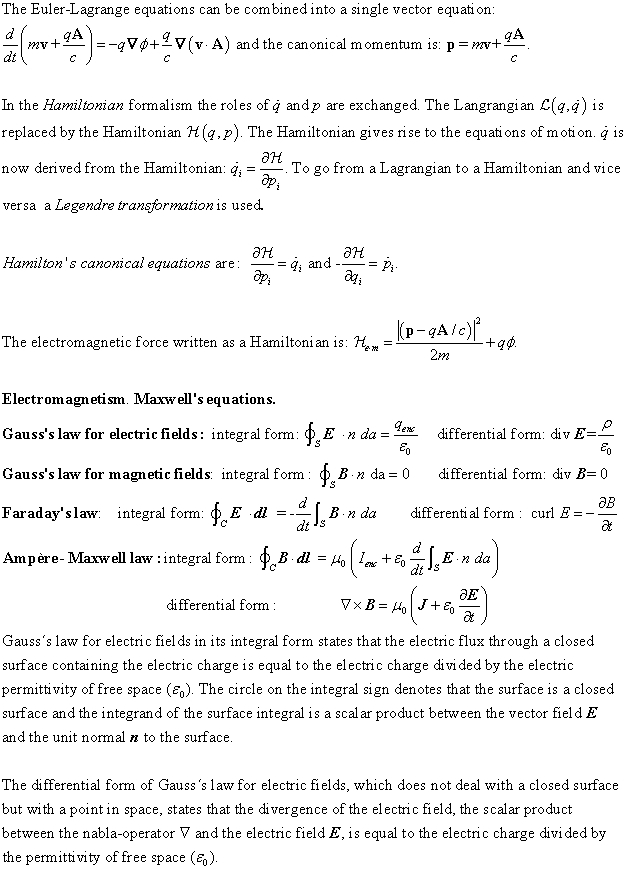

X-rays, gamma-rays. Gamma radiation (related to the decay of the atomic nucleus in radionuclides) and X-ray (related to retardation of electrons and also to tightly bound electrons which have been excited to higher bound states which emit x-ray radiation when reverting to their original states, "characteristic x-ray radiation") are ionizing radiation with the ability to damage DNA leading to cancer. Gamma radiation and X-rays has the necessary penetration for NEE.
Units. Exposure to radiation is measured in roentgen, the ability to deliver 8.75 mJ of energy to 1 kg of dry air in specified conditions. The unit does not give any information on whether the energy is absorbed or not. The gray (Gy) measures the energy which the object absorbs from any type of radiation. If the absorbed dose is 1 J/kg, then one gray of ionizing radiation has been absorbed. Different kinds of ionizing radiation have different biological effects. The Sievert (Sv) is a measure of dose equivalent. The dose in Sv is equivalent to the absorbed dose (in gray) multiplied by the RBE (relevant biological effectiveness) factor. RBE ≈ 1 for x-rays, gamma rays and electrons.
Wave-matter interaction. Interaction of radiation with matter is described by, among many others, Nikjoo, Uehara and Emfietzoglou (58). X-rays which do not penetrate biological tissue in a linear straight path are scattered or they are absorbed giving rise to the photoelectric effect. When the energy of the X-ray photon increases above the binding energy of the K-shell electron the probability of absorption of the x-ray photon increases as the X-ray photon now has sufficiently high energy to release the K-shell electron4 from the atom, the "K-edge". When the energy of the X-ray photon increases further above the binding energy of the K-shell electron the probability of the photoelectric effect diminishes, the probability is proportional to 1/E3 ("E" is the energy of the X-ray photon). The probability of photoelectric absorption increases with the atomic number, Z, and is proportional to Z3 (59).
An electron which performs a transition to an empty state with lower energy can either give rise to characteristic X-ray radiation or use the energy difference to cause another electron to leave the atom giving rise to an Auger electron, an example of autoionization (60).
Coherent scattering (Rayleigh scatter) is the scattering of the x-ray photon by the atom without energy loss (elastic scattering). For soft tissue, the photoelectric effect and Compton effects are equal at 25 keV. For bone, the photoelectric effect and Compton effect are equal at 40 keV (59).
Triplet production occurs in the field of the electron instead of the field of the nucleus. Three particles appear: the positron, the created electron and the original electron. The threshold for triplet production occurs at twice the threshold for pair production, 2.04 MeV.
Attenuation coefficients. The linear attenuation coefficient (μ) is the fraction of the incident photons removed from the beam (through interactions with the tissue, that is, Rayleigh scatter, Compton scatter and the photoelectric effect) in travelling one unit of distance, it is measured in cm-1.
X-rays with the same frequency are absorbed by the tissue according to the formula N = N0e-μt. N0 is the number of photons incident on an absorber of thickness t (cm), N is the number of photons transmitted, and μ (cm-1) is the attenuation coefficient. For soft tissue μ is 0.38 cm-1 at 30 keV and 0.21 cm-1 at 60 keV. For bone μ is 1.6 cm-1 at 30 keV and 0.45 cm-1 at 60 keV.
If a 60 keV X-ray beam traverses 5 cm of soft tissue the calculation N = N0e-0.21x5 ↔ N/ N0 = e-0.21x5 ↔ N/ N0 = e-1.05 = 0.35 shows that 35 % of the photons have traversed the tissue without interacting with it and that 65% of the photons have interacted with the tissue.
The equation N = N0e-μt is valid only if the attenuation coefficient is a constant which is true only if the photons in the incident beam all have the same energy and if the beam is narrow. If the beam is not narrow the probability that photons will be scattered in the attenuator making them reach the detector will increase. In the case the beam is not narrow the attenuation curve is described by the equation N = N0e-μt B(x, hv, A, L) where B, a photon buildup factor, is dependent on x, the thickness of the attenuator, hv, energy of the photons, A, area of the attenuator, and L, the distance between the attenuator and the detector (61).
The mass attenuation coefficient is the linear attenuation coefficient (μ) divided by the density of the tissue in question. It has the dimension m2/kg (59). The electronic attenuation coefficient eμ has the dimension m2/electron and the atomic attenuation coefficient has the dimension m2/atom. These three attenuation coefficients are often called cross sections.
For soft tissue and the lowest energies, the largest part of the attenuation is caused by the photoelectric effect, at higher energies the most attenuation is because of Compton scatter. It is found experimentally that the absorption cross section is proportional to the fourth power of the nuclear charge Z and the third power of the wavelength λ.
The energy transfer coefficient μtr is defined as μtr = μ(Etr/hv) where Etr is the average energy transferred per interaction. The energy transferred in Δx is ΔEtr = μtrNhv Δx where N is the number of photons reaching the layer Δx.
The energy absorption coefficient μab is defined as μab = μ(Eab/hv) where Eab is the average energy absorbed per interaction. The energy absorbed in Δx is ΔEab = μabNhv Δx. The Compton energy transfer coefficient σtr is defined as σtr = σ(σEtr/hv) where σ is the Compton cross section and σEtr is the mean energy set in motion, the latter gives the energy transferred to kinetic energy in the Compton process making it available for absorption.
For energies larger than 1.02 MeV the X-ray photon can produce an electron positron pair, it involves an interaction between a photon and the nucleus (61). The high energy electrons and positrons produced in a pair process have sufficient energy that some of it is converted into radiation by bremsstrahlung and escapes.
The total attenuation coefficient, μ, is the sum of the four components: μ (total) = T (photoelectric) + σcoh (coherent) + σinc (Compton) + K (pair) related to the photoelectric effect, coherent (Rayleigh scatter), Compton scatter and pair production respectively. With relevant subscripts this equation also applies to the mass, the electronic and the atomic attenuation coefficients.
The spatial distribution of ionizing effects varies between different kinds of radiation. A low-energy electron set in motion by diagnostic x-rays produces ionization well separated in space, x-rays are sparsely ionizing. An electron set in motion by cobolt-60 gamma rays is even more sparsely ionizing. Higher energy of the particle causes the density of the ionizations to be lower. A relevant concept is linear energy transfer (LET) which is the energy transferred per unit length of the track. LET is an average value, energy deposited per unit length of track has a large variability. The higher the energy of the particles the lower is the LET-value, i.e. the biological effect is lower (62, 63).
Biological effects of radiation are to the greatest extent caused by damage to DNA (deoxyribonucleic acid). This damage to DNA is brought about through direct action and indirect action (62). In direct action the absorbed X-ray photon causes an electron to eject from the atom which has absorbed the x-ray photon and this ejected electron interacts with DNA in a damaging way.
In indirect action the ejected electron interacts with for instance a water molecule to produce a hydroxyl radical which causes the damage to the DNA. Indirect action is dominant for sparsely ionization radiation (low LET-value) such as X-rays (62).
SH compounds which are the most efficient radioprotectors have a straight chain of two to three carbon atoms with a free, or potentially free, SH group at the one end of the carbon chain and a strong basic group such as amine or guanidine at the other end of the carbon chain (62). SH compounds are efficient radioprotectors against radiation with low LET-value (X-rays, gamma rays). The mechanism for the radioprotection are free-radical scavenging and hydrogen atom donating which facilitates chemical repair of DNA-damage. Additional mechanisms of protection are suspected but not known.
Amifostine is approved by the U.S. Food and Drug Association (FDA) for the use in radiation therapy to prevent xerostomia in patients treated for head and neck cancer (trade name Ethyol). Amifostine is a prodrug which is dephosphorylated by the enzyme alkaline phosphatase permitting it to enter cells through facilitated diffusion where it scavenges free radicals generated by ionizing radiation.
Melanin and nanoparticles have been used to reduce damage to tissues caused by ionizing radiation (64) (65) (66) as well as other substances (67).
Gamma radiation is used in Gamma Knife Neurosurgery, mostly for the treatment of brain tumours by producing tissue necrosis (68). The radioisotope used is 60Co, which has two radioactive breakdown pathways giving rise to radiation with energy of either 1.17 or 1.33 MeV. 192 beams are used, they are cross-fired meaning that they meet exactly at the target. The patient's head is moved in order to have the whole target irradiated. The required movement of the patient's head is performed by a robot, APS, "Automatic Positioning System". The collimators (a collimator narrows a beam of particles or waves and can vary the angular spread) for the beams are 4, 8 and 16 mm in diameter. The target dose of radiation is not homogenous because of technical reasons. Mechanical accuracy is < 0.3 mm.
Over 500,000 patients have been treated for over 25 years. The risk of gamma knife induced cancers is not known. Current estimates are between 1 and 2% at 20 years and 0.005% to 0.1%.
Radiosurgery using X-ray can be used both inside and outside the cranium (69). Built in X-ray imaging and MR, PET-scanning and ultrasound is used for imaging guiding of the treatment. Image axes can be oblique or perpendicular to the treatment beam axis. To correct for MRI distortion, which can be caused by inhomogeneous magnetic field, ferromagnetic materials, spatial variations in magnetic susceptibility and nonlinear magnetic field gradients, fusion of MRI and CT of the same patient can be used. The Tomotherapy Hi-Art system is combined with a CT-scanner and delivers treatment in a helical fashion with movement of the beam relative to the patient as in CT-scanning. High-definition multileaf collimators (micro-MLCs) with leaf sizes 2.5 - 3 mm are used for beam shaping. The shape of the aperture and the fluence (number of photons passing a specified area per specified time) within the field can be varied.
The ExacTrac® system automatically aligns the target volume with the treatment beam using infrared tracking markers on the external body and anatomical registration of bony structures through X-ray imaging. The Novalis and Novalis TX has a IR tracking system that updates marker positions every 50 ms or less and monitors the real-time position of patient and table. Implantation of radiopaque markers are used when soft tissue targets are not closely related to skeletal landmarks.
Improved imaging makes systems of immobilization of the patient through for example Electa Stereotactic Body frame unnecessary. When calculating the dose of X-ray in a given treatment the photon interactions (photoelectric absorption, Compton scatter and pair production) are simulated as well as the transport of photons, electrons and positrons with MC-simulation (Monte Carlo simulation) (70).
Assume that in NEE the area of the proximal portion of the femur of interest is about 1 dm2 = 100 cm2, to have an even figure and something to calculate with, and the surface of the proximal part of the femur covered by a CFU on average is 0.5 cm x 0.5 cm = 0.25 cm2, that would mean 100 cm2/0.25 cm2 = 400 CFUs. Assume that the focusing of 10 beams are used, giving 10 x 400 = 4000 beams at the start of a step of the treatment, which is multiplied by the number of steps, for example 10 steps, which gives 40000 beams. That is a lot of beams and in addition there are the CFUs for the acetabulum. Tens of thousands of beams give concern about damage caused by ionizing radiation. The size of the CFUs may be smaller at the interface between different kinds of volume (deficit, redundant, intermediate). With a flattened femoral head viewed in the antero-posterior direction, in abduction there would be a reduced contact area between the medial part of the femoral head and the medial part of the acetabulum and vice versa, in adduction there is a reduced contact area between the lateral part of the femoral head and the lateral part of the acetabulum. Every CFU does not need to be irradiated with the hip joint in the same position. The demand to discriminate between different kinds of volume would make the CFUs smaller near the boundaries between different kinds of volume but would allow the CFUs to be larger within confluent areas of the deficit and the redundant volumes. On the other hand, a larger volume of a CFU could also encompass a larger portion of the bone marrow.
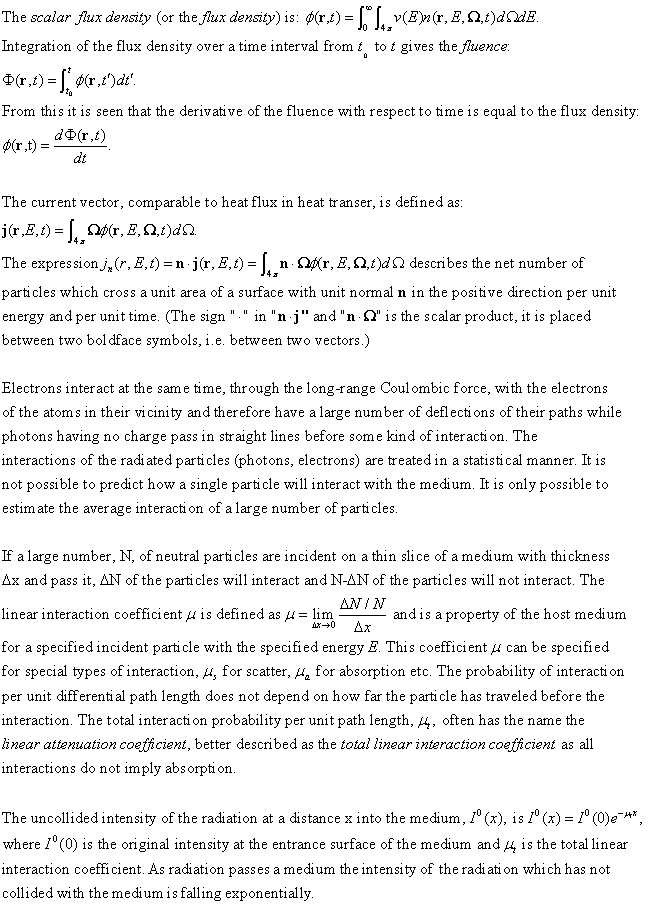
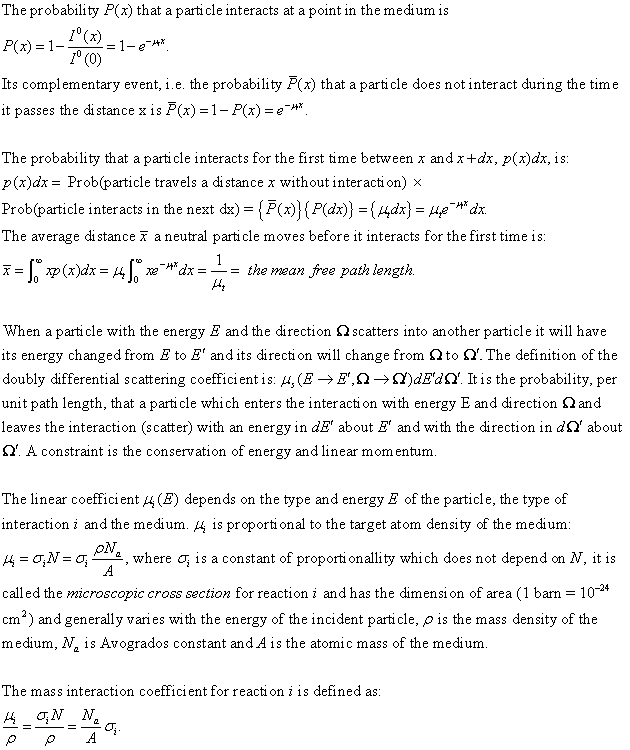
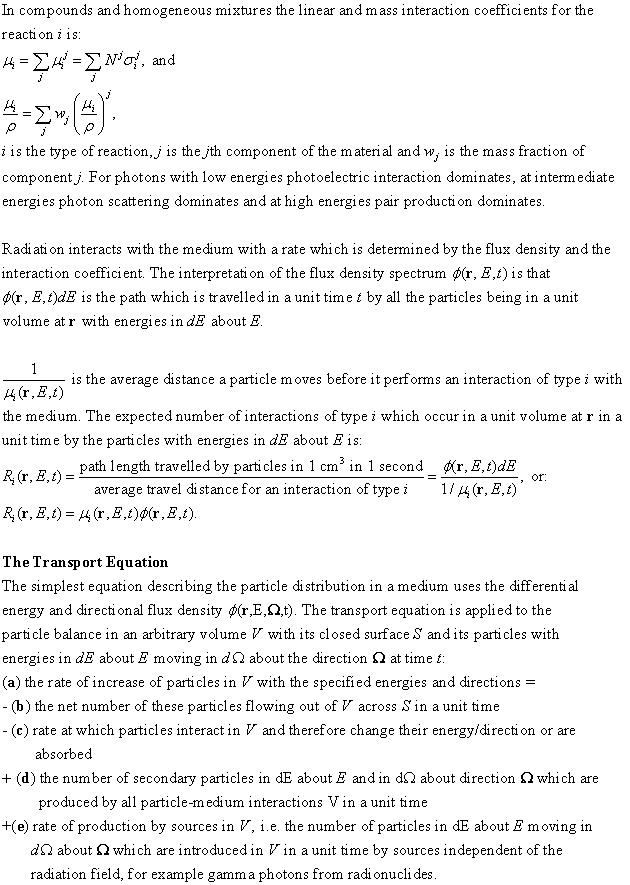

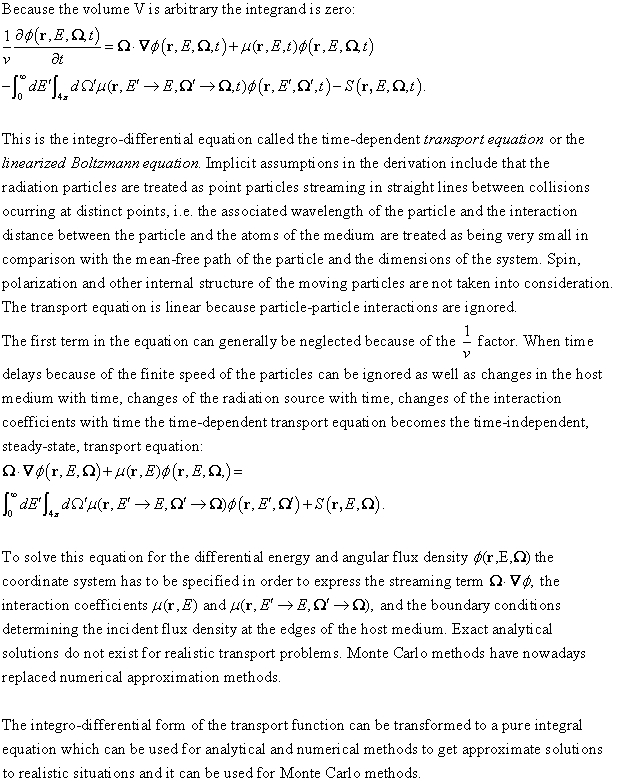




Synchrotron radiation is used for imaging (74) and can be used for treatment.
In Microbeam Radiation Therapy (MRT) an array of beams with 50 micrometre thickness and 200 micrometre centre to centre distance is used (75). The beams used in hospitals are from several mm to centimetres wide.
Minibeams (75,76) are constructed by a high energy white-beam chopper which consists of a series of ten tungsten carbide blades with thickness 6 micrometres. The beam thickness is 600 micrometres and the inter-beam separation also is 600 micrometres. Two sets of beams can be orthogonally interlaced or several beams can be radiated from different angles.
An advantage with narrow beams such as microbeams and minibeams is that they spare healthy tissue before and after the tumour, because of rapid biological repair by cells in the nonirradiated slices of tissue. Studies have shown that this sparing effect in the rat central nervous system is present for beams up to 0.68 mm thickness. Minibeams are not so sensitive to cardiosynchronous pulsations as microbeams are.
By changing the parameters in the setup of the minibeams the width of the beams can be varied. The intensity of a beam produced at a synchrotron can be varied.
A scintillator is a substance, organic or inorganic, which when irradiated by ionizing radiation emits light in the visible or UV-region (77). Inorganic scintillators have high light output and linearity but often are slow in their response time. Organic scintillators generally have a shorter response time but a lower output.
The search for scintillators began immediately after the discovery of X-Rays in 1895. Ordinary photographic film was not suitable to detect X-Rays. The first scintillator which was used was CaWO4 in 1896.
Fluorescence is the immediate emission of visible radiation from a substance as a consequence of its excitation. Phosphorescence is the emission of light with a longer wave length than fluorescence and often is emitted slowly. Delayed fluorescence has the same wave lengths as prompt fluorescence but is slower.
Scintillators are used for detection of particles and radiation in high energy physics, to detect radioactive material at country borders ("homeland security") and in medical imaging (planar X-ray imaging, positron emission tomography (PET), X-ray computerized tomography (CT) and single-photon emission tomography (SPECT)).
Inorganic scintillators. In insulators and semiconductors electrons can be found in discrete bands of energy. The valence band represents the electrons bound at lattice sites. The electrons which have enough energy to freely migrate throughout the crystal are located in the conduction band. In a pure crystal the electrons cannot be found in the intermediate band of energies, the forbidden band. An electron in the valence band can be elevated to the conduction band through the absorption of energy, leaving a hole in the valence band. The return of the electron to the valence band from the conduction band with the emission of a photon is an inefficient process in the pure crystal.
Small amounts of impurities, activators, are added to inorganic scintillators to increase the probability that the de-excitation process emits a photon. The addition of activators creates energy levels within the forbidden band. The de-excitation sites created by the activators are called luminescence centres or recombination centres. Ionizing radiation will cause many electron-hole pairs through the elevation of electrons from the valence band to the conduction band. The positive hole will move to an activator and ionize it, the energy of a lattice site is greater than the ionizing energy of the activator. At the same time the electron migrates through the crystal until it encounters an ionized activator. The electron then can move into the activator site and a neutral configuration is formed. The activator state which is formed when the electron moves into it can be an excited state and if the transition to the ground state is allowed it will de-excite fast and emit a photon. If the de-excitation to the ground state is not allowed it may require more energy, for instance through thermal excitation, to acquire a higher energy state wherefrom it can de-excite to the ground state. The light is emitted slowly and is called phosphorescence which can be the cause of background light or afterglow in a scintillator. De-excitation of an excited state can also occur without radiation, quenching.
Instead of moving independently the electron and the hole can move in a configuration called an exciton. An exciton can move to an activator atom and cause similar activated configurations which can de-excite to the ground state and emit light. The doped crystal (a crystal containing activator sites) can be transparent to its own scintillator light. Events like these in a solid crystal is a topic in solid state physics.There are many kinds of inorganic scintillators: various alkali halide scintillators; other slow inorganic crystals: bismuth germanate, cadmium tungstate, zinc sulphide, calciumfluoride, strontium iodide; inactivated fast inorganics with low light yield: bariumfluoride, pure cerium fluoride, cerium halides, lead tungstate; cerium-activated "fast" inorganics: rare earth oxyorthosilicates, lanthanoid pyrosilicates, rare earth aluminium perovskites, rare earth aluminium garnets, lanthanum halides, lutetium halides and elpasolites; transparent ceramic scintillators; glass scintillators and noble gas scintillators. Some of them can be used in gamma ray spectroscopy, especially those with a high Z element which gives a larger cross-section for the photoelectric effect related to x-rays and gamma rays. Some inorganic scintillators are hygroscopic and must be protected from water. If radioactive isotopes are present a background activity will be the result (77). The thesis of Birowosuto (78) describes the development of several Ce3+- doped scintillators, the theory behind it and instruments used.
Ceramic scintillators. A glass ceramic composite consists of small crystallites which are embedded within a glass matrix. They may be very useful for instance in medical imaging and in homeland security applications (79).
Thin film scintillators. Thin film scintillators can be produced down to submicron thickness. They are not suitable for detection of gamma- or hard (high-energy) X-rays because of the higher penetration depth of these rays (79). This is the same principle which makes a targeting system with beams and conjugates containing scintillators in NEE impossible. A scintillator must have a certain thickness, the absorption takes place somewhere in the scintillator but to ensure absorption the thickness cannot be too low. A single scintillator molecule would be comparable to a thin film scintillator where the thickness of the scintillator becomes smaller and smaller and in the limit the thickness of the thin film scintillator will only be the thickness of a molecule.
Fluorescence in organic scintillators is caused by transitions in the energy level structure of an individual molecule independent of its state of aggregation (solid, liquid, gas). This can be compared to crystalline inorganic scintillators, for example sodium iodide, which needs a regular crystal lattice for the scintillation process. Sodium iodide dissolved in water does not scintillate when irradiated by ionizing radiation.
Many organic scintillators have a π-electron structure as a result of symmetry properties. The energy diagram of an organic scintillator has singlet states (spin 0) labelled S0, S1, S2, ... and triplet states (spin 1) T1, T2, T3, ... Each of the electronic levels is subdivided into a finer spacing corresponding to vibrational states of the molecule. The higher singlet electronic states caused by ionizing radiation are immediately de-excited to the S1 electron state by radiationless internal conversion. States with vibrational energy are not in thermal equilibrium with its neighbours and quickly lose its vibrational energy. Prompt fluorescence is caused by a transition between the S10 state (lowest vibrational state of the S1 state) and one of the vibrational states of the ground electronic state.
The first triplet state T1 has a longer duration than the singlet state S1. Through the transition intersystem crossing some excited singlet states may be changed into triplet states. As the T1 state has a longer duration the light emitted from the transition from T1 to S0 is a delayed emission, phosphorescence, which has a longer wavelength than fluorescence because the T1 state lies below the S1 state in the energy diagram. Molecules in the T1 state can be excited back to the S1 state by heat and then have a transition to the S0 state giving rise to delayed fluorescence.
Except for the S10 - S00 transition fluorescence has a longer wave length than needed for absorption with the consequence that the scintillator can be transparent to its own fluorescence emission, there is only a small overlap between the absorption and emission spectra (Stokes shift).
The scintillator efficiency is defined as the proportion of incident energy transformed to visible light (the definition is also applicable to inorganic scintillators). Quenching are de-excitation processes that do not emit light. "Binary" organic scintillators consist of a small concentration of a scintillator in a solvent where the solvent molecules can transfer energy from the ionizing radiation to the scintillator. Sometimes a third component is added which functions as a "wave-shifter" absorbing the light emitted by the scintillator and radiating it with a longer wave length.
Organic scintillators are crystals, liquid and plastic. In many liquids oxygen is a strong quenching agent reducing fluorescence efficiency. Organic liquid and plastic scintillators are often used as "binary" compositions. Organic scintillators can be "loaded", addition of high Z elements to increase the photoelectric cross section for gamma rays. Without high Z elements such as lead or tin organic scintillators have no photopeak when exposed to gamma rays but only a Compton continuum. Decay time describes the prompt scintillation yield from organic scintillators (77).
A nanocomposite scintillator consists of nanometre material embedded in a solid matrix. There are three classes of them, organic scintillating nanoparticles in an organic matrix, inorganic scintillating nanoparticles in an organic matrix and inorganic scintillating nanoparticles in an inorganic matrix (79).
Once again, in applications scintillators more often than not have macroscopic dimensions. That is not the case in NEE where one or a limited number of scintillator molecules are used and such a scintillator suitable for NEE does not exist.
With the conjugate with one kind of scintillator and an adjacent photoswitch present in the whole systemic circulation the application of a beam of ionizing radiation will activate the conjugate along the entire path of the beam. If two or more beams are used and focused at a point the concentration of the activated conjugates will be higher at the focus of the beams compared to the concentration along each of the beams outside the focus. Targeting in the sense that there should be no activated conjugates outside the focus is not fulfilled.
The only way to circumvent this problem is to use a conjugate with two kinds of photoswitches, P1 and P2, each with a scintillator attached to it, S1 and S2, which in turn responds to a wavelength/polarization of the ionizing radiation being separate from the activating wavelength/polarization of the other scintillator. The two photoswitches must simultaneously be activated in order for the conjugate to enter the cell.
This means that two sets of beams of ionizing radiation must be used, B1 and B2, each with its own frequency/polarization. Both of these two sets of beams of ionizing radiation will be focused at the intended point (CFU). Along the entire path of each of the beams of ionizing radiation belonging to the two sets only one type of photoswitch will be activated. The only place where there are conjugates with both types of photoswitches activated is the focus of the two sets of beams. Targeting is thus fulfilled.
The conjugate must have two photoswitches, each with its own scintillator which is activated by the frequency/polarization of the ionizing radiation of one but not both of the two sets of beams. The function of the conjugate to enter the cell and its nucleus must depend on the simultaneous activation of both photoswitches of the conjugate.
In NEE a conjugate has six components, two scintillators, S1 and S2, two photoswitches, P1 and P2, a switchable cell-entry function which enables the conjugate to enter the cell of interest and a promotor which is removable from the genome in the presence of a detaching molecule. The function of the scintillator is to transfer part of the absorbed energy to the photoswitch causing it to alter its stereochemical configuration. Within the boundaries of a CFU several processes are to take place, the excitation of the two scintillators by ionizing radiation resulting in the activation of the two photoswitches, the uptake of the conjugate by the relevant cell, the transport of the conjugate through the cytosol into the nucleus, the attachment of the promotor to its correct site in the genome and the start of transcription of the gene of interest. The excitation of the scintillators must occur before the focusing beams of ionizing radiation have been turned off. The binding of the conjugate to the receptor on the cell membrane must occur before the circulation, or diffusion, has transported the conjugate out of the CFU, that is the excitation of the scintillators and the ensuing excitation of the photoswitches must be instantaneous or at least so rapid to fulfil this goal and to ensure that the distribution of activated conjugates within a CFU is homogenous (the rate constants of the relevant biophysical and biochemical reactions must be high enough) and the excited state of the two photoswitches must be short enough in order to avoid the presence of activated conjugates outside the intended CFU.
In addition to the difficulty of creating scintillators which can absorb ionizing radiation and transfer part of the absorbed energy to photoswitches which will cause the transformational change of the photoswitches there is the problem of interference because of wave-matter interaction, i.e. the problem of keeping the two channels B1 - S1-P1 and B2 - S2 - P2 separate from each other. The absorption curve of one kind of scintillator should only encompass the frequency of its intended set of beams and not the other set of beams. A photon belonging to a beam with the higher of the two frequencies could after interaction with an atom cause activation of a scintillator having an absorption curve encompassing a lower frequency. The beam with the higher frequency could excite an electron in an inner shell of a nearby atom and when this electron reverts to its ground state characteristic x-ray radiation will be emitted, if the frequency of this photon is inside the absorption curve of the non-intended scintillator it will be activated. Another mechanism of such an interference is Compton scattering where the incoming photon delivers part of its energy to the electron. There must be a two-channel system where the two channels do not interfere with each other.
Concerning neighbouring CFUs the different kinds of volumes are located in confluent areas, it is not the case that if following a straight line projected onto the surface of the femoral head one will encounter first a CFU belonging to the redundant volume, then a CFU belonging to the deficit volume, then a CFU belonging to the redundant volume and so forth. A CFU selected at random will most probably as its neighbours have CFUs that belong to the same category of volume because the different kinds of volumes are confluent. A conjugate which because of the thermal relaxation time of the photoswitches has its effect in a neighbouring CFU is not a drawback as long as the neighbouring CFU belongs to the same category of volume. Where it matters is at the boundaries between different categories of volumes and if activated conjugates should enter the systemic circulation outside the treatment volume.
Comparison between ionizing radiation in NEE and radiotherapy/X-ray imaging. Differences between the mechanism of action of the beams of ionizing radiation used in NEE and for radiotherapy is that in NEE the purpose of the beams is to be absorbed by the scintillators of the conjugate, in the case of radiotherapy the beams are used for the purpose of causing tissue necrosis and that in NEE targeting is achieved by using two sets of beams with different frequencies/polarization states with the result that the desired molecular state, the activated conjugates, occurs only at the focus of the two sets of beams but not along each beam belonging to the two sets whereas in radiotherapy the desired molecular state, the radicals, occurs along the entire length of each of the participating beams. Compared with radiotherapy NEE gives the opportunity to achieve a more varied spectrum of chemical reactions occurring at the focus depending on what the isomerization of the photoswitches initiates, radiotherapy only gives rise to radicals and free electrons through the photoelectric effect.
A difference between the mechanism of action of the beams of radiation used for NEE and for radiotherapy on the one side and x-ray imaging on the other side is that in the former case the completion of the mission of the beams is at the object inside the body whereas in the latter case there is no intended chemical action inside the body but instead the completion of the mission of the beams is achieved when the beams reach the x-ray detector located outside the body.
In NEE the overall entity is the three-dimensional surface, that is the surface bordering on a deficit or redundant volume, in x-ray imaging the overall entity is the image. For NEE the smallest unit of the surface is contained within the three-dimensional CFU and in x-ray imaging the smallest unit of the image is the two-dimensional pixel. In NEE the size of the CFUs and their time of activation could vary over the surface but in x-ray imaging the pixel size in the image is constant and the pixels are activated practically at the same time.
Because soft tissue and bone have different attenuation coefficients (μ) there is a difference if a beam of ionizing radiation on its way to the intended CFU ("point") passes through bone or not. A "direct point" is a point where none of the focusing beams of the two sets traverses bone and an "indirect point" may arbitrarily be defined as a point where at least one of the focusing beams traverses bone. A "point" in this context can be regarded as a CFU.
Whereas the necessity for a beam to traverse bone (because of anatomical reasons) presents the problem of attenuation of the beam including scattering the problem of a boundary between different kinds of volumes (deficit, intermediate and redundant) presents the problem of having unwanted effects in the vicinity of the intended CFU. A "boundary point" is a point which lies at the boundary between two different categories of volume (deficit, intermediate, redundant). When acting as a focus of targeting beams the risk is that unwanted effects will arise at the other side of the boundary. An "internal point" is a point which is situated inside the boundary at such a distance that there is no risk of getting unwanted effects on the other side of the boundary. The magnitude of the distance is dependent on what the promotor achieves. If the promotor causes the production of a growth factor diffusing into the surroundings the distance is the diffusion distance. If that would be the case another complication could arise, if a growth factor diffuses outside the cell it could enter the systemic circulation and then the treatment would not be targeted, any possible adverse effects the growth factor might have on the whole body would then have to be considered. It is not only the ON-signal with ionizing radiation which must be targeted, also the effects of the signal must be targeted.
Absorption maxima for photosensitizers (PS) currently in market or in clinical trials are between 630-796 nm (80). Depending on the physicochemical properties (charge, hydrophobicity) different photosensitizers have different preferences as regards their distribution in the cell (cell membranes, cytoplasm, nucleus). Photosensitizers can be linked to other types of molecules, for example monoclonal antibodies. The linkage is of the type peptide, isothiocyanate, disulphide or hydrazone. A linker between the photosensitizer and the other molecule can also be used: poly-L-glutamate, poly-L-lysine, dextran, hydroxypropyl methacrylamide, albumin. Another approach is to link the photosensitizer to a molecule which is transported into the cell by receptor-mediated endocytosis. Examples of molecules which have been used for this purpose are transferrin (transport protein of iron in serum) and LDL (Low Density Lipoprotein).
Photosensitizers have been conjugated to EGF (Epidermal Growth Factor) where the carriers have been dextran, polyvinylalcohol and human serum albumin; to gonadotropin-releasing hormone (GnRH) receptor agonist; to GnRH antagonist; to the simian virus SV40 large tumour antigen nucleus localization signal (NLS) in order to deliver the photosensitizer to the nucleus; to the alpha(V)beta(3) integrin specific peptide RGD (H-Arg-Gly-Asp-OH) motif that binds to alpha(V)beta3 integrins present on tumour microvascular endothelial cells; to a vascular receptor endothelial growth factor receptor-specific heptapeptide [H-Ala-Thr-Trp-Leu-Pro-Pro-Arg-OH(ATWLPPR)] (in addition to the three letter abbreviations for amino acids there are also one letter symbols for them, "A" is for Alanine, "T" for threonine, "W" for tryptophan, "L" for leucine, "P" for proline and "R" for arginine) via the spacer 6-aminohexanoic acid (Ahx) where this conjugate was found to bind to neuropilin-1; to a membrane-penetrating arginine-oligopeptide (R7) with enhanced intracellular uptake of the photosensitizer (5-[4-carboxyphenyl]-10,15,20-triphenyl-2,3-dihydroxychlorin (TCP) as a result. Photosensitizers have been conjugated to smaller molecules such as folic acid, steroid hormones and saccharides. The purpose is to use membrane bound receptors for these small molecules to achieve intracellular uptake of the photosensitizers.
Nanoparticles have been used in photodynamic therapy. There are three main classes of them, one is photodynamically active itself, the second class acts as an "energy transducer", they absorb light and transfer the energy to a photosensitizing molecule. The third class acts as carriers for conventional photosensitizers. In this context "nano" is defined 1-100 nm. An example of nanoparticles used as direct photosensitizers are quantum dots (Qdots), which are composed of semiconductor materials (CdSe, InP, InAs), often with a core of one material with a surrounding shell of another material. The surface of these Qdots can be stabilized and ligands, for instance peptide sequences, can be attached to the surface to target cell receptors.
In the second class, nanoparticles used as energy transducers, a Qdot is conjugated to a photosensitizer molecule. The light is absorbed by the Qdot and resonant energy is transferred to the photosensitizer molecule raising it to an excited singlet state, allowing more flexibility in selecting the spectral properties of the PS so that its other properties can be improved. Problems concern toxicity of heavy metals in the Qdots and in vivo delivery.
The third class of nanoparticles, used as carriers, can have a load of PS, including hydrophobic drugs, either encapsulated in the nanoparticle or attached to the surface. The advantage is that the Qdot can have a high payload.
X-ray induced luminescence in nanoparticles. Nanoparticles have been produced which exhibit scintillation luminescence or persistent luminescence when irradiated by X-rays (81). The photosensitizers are coated onto or attached to the nanoparticles. As the nanoparticle's emission spectrum is dependent on its diameter it is possible to adjust it to the photosensitizer's absorption spectrum. Nanoparticles with a higher atomic number have higher luminescence efficiencies. Examples of such nanoparticles are BaFBr:Eu2+,Mn2+ (the crystal has been doped with, supplemented with, a small amount of the elements which follow after the colon), which has emission bands at about 400, 500 and 640 nm, and LaF3;Ce3+ which has emission bands at 350 nm and tailing at 500 nm. Persistent luminescence means that the luminescence continues a few minutes to tens of hours after the X-ray radiation has ceased. This may shorten the required time for activation of the photosensitizers by X-ray exposure from 30 to 10 seconds. The emission spectrum of the donor must overlap the absorption band of the acceptor and the distance between the donor and acceptor should be less than 10 nm. A method for linking photosensitizers such as porphyrins to nanoparticles is the EDC/NHS reaction (EDC: 1-(3-Dimethylaminopropyl)-3-ethylcarbodiimide, NHS: N-hydroxysuccinimide).
In a biological application a "caged" molecule is a molecule with a function which is linked to a photosensitive molecule, "photoremovable protecting group" (82). Because of the bond with the photosensitive molecule the function of the biomolecule is lost, the site of the bond on the biomolecule is chosen to achieve this loss of function. When the conjugate between the biomolecule and the photosensitive molecule is exposed to light the bond is broken and the biomolecule regains its normal function. A caged molecule can be used as a phototrigger.
There are several types of photoremovable protecting molecules: 2-nitrobenzyl, its 4,5-dimethoxy analogue (DMNB), 1-(2-nitrophenyl) ethyl (NPE) and its 4,5-dimethoxy analogue (DMNPE), the α-carboxy-2-nitrobenzyl (CNB) groups, coumarin-4-ylmethyl groups, β-hydroxyphenacyl (p-HOC6H4COCH2, pHP) and benzoin (Bnz).
Classified according to functional group biomolecules and ions which have been targeted are carboxylates, amines and amides, alcohols and phenols, phosphates, protons, calcium and carbonyl compounds (aldehydes, ketones). Molecules which have been caged include nucleotides (AMP, ADP, ATP, 8-bromo-cAMP, cGMP, CDB (cytidine-5'-diphosphate), DNA, RNA, mRNA) , nicotinamide coenzymes (NAD, NADP), sphingosinphosphate, carbamylcholine, galactose and phenylephrine. Proteins and peptides which have been caged include colifin, thymosin β4(Tβ4), G-actin, transcription factors, the heptapeptide C-kemptide, channels and pores (α-haemolysin, nicotinic acetylcholine receptor (nAChR)), selfsplicing proteins, neuropeptide Y, nuclear localization signal, p21ras, antibody (against brain-derived neurotrophic factor (BDNF)), neurotransmitters (α-glutamate, GABA, glycine), various enzymes including protein kinase (PKA), protein phosphatases, papain, chymotrypsin, HIV-1 proteinase, β-galactosidase, choline esterase, ribonuclease, and lysozyme T4. With the introduction of the unnatural amino acid o-nitrophenylglycine (Npg) the cleavage of the backbone of the protein is achieved when exposed to light.
To minimize damage to proteins and nucleic acids a wavelength above 350 nm is used. Desired physicochemical properties of the caged molecules are water solubility, resistance to hydrolysis and non-toxicity. The quantum yield is the proportion of molecules that undergo photolysis to form the desired photoproduct after absorbing a photon. The introduction of methoxy groups in the benzene-ring of the photosensitive molecule may shift the absorbance to higher wave lengths but also result in a lower quantum yield. The photochemical release should be efficient and the departure of the substrate from the protecting group should be a primary photochemical process occurring directly from the excited state of the protecting group. By-products of the photorelease which may be produced should not absorb the light of excitation, not interfere with the biological system and have a fast release relative to the studied process.
Photochromism is defined as the photoinduced reversible transformation of a molecule, a photoswitch, between two stable states associated with a change in absorption spectra. In T-type photochromism one isomer is thermodynamically unstable and the compound spontaneously reverts to the original state. P-type photochromism implies that both the isomers are thermodynamically stable and conversion from one isomer to the other must be carried out by irradiation in both directions. Examples of photoswitches are indolinooxazolidines (IndOxA), azo compounds, diarylethenes and spiro-compounds (83).
A phototrigger (caged molecule) cannot be used for the photoswitchable entry of conjugates into the cells because the reaction is not reversible, the ability of the conjugate to enter the cell should only be present within the irradiated CFU and not outside it. What is needed is a photoswitch (82) which reversibly changes its conformation when its attached scintillator is irradiated by a specific wave length/polarization of ionizing radiation and keeps this transformed state long enough to enable the conjugate to enter the cell but spontaneously reverts to its original state (T-type photochromism) fast enough to avoid the existence of the transformed state outside the intended CFU fulfilling the requirement of targeting.
Azobenzene is changed from trans to cis configuration when exposed to light with a wavelength λ = 320 nm with a concomitant change from a plane to a nonplanar structure. cis-Azobenzene has absorption peaks at 440 nm, 280 nm and 250 nm. The absorption curves of cis- and trans-azobenzene are overlapping. The half-life for thermal cis-to-trans isomerization of unmodified azobenzene is about 3-4 days at room temperature. Exposure to light produces at most ~80% cis or ~95% trans isomers. Thermal relaxation of the cis form produces a higher percentage of the trans isomer, > 99%, when stored in the dark at +50 ℃ (84,85,86). In an ordinary equilibrium reaction the concentration of the product (reactant) is never zero. In NEE, a nonzero concentration of activated conjugates in the systemic circulation will risk the spread of the activated conjugates throughout the skeletal system and possibly the uptake of the conjugates into other cell types too.
Behamy and Woolley have reviewed azobenzene photoswitches for peptides, proteins, ligands, nucleic acids, molecules that interact with DNA or RNA, oligonucleotides, lipids and carbohydrates (87). Substitutions on the phenyl ring can influence the rate of thermal cis-to-trans relaxation. In general, red shifted azobenzenes have faster thermal relaxation. Substitutions at positions ortho to the azo group can exhibit steric effects on azobenzene properties that are not seen with similar meta or para substituted derivatives.
The half-life of cis-azobenzene can be decreased because of its chemical environment. Pozhidaeva et al (88) designed a series of methanethiosulfonate (MTS)-bearing thiol-reactive azobenzene-based cross-linkers. The linkage between the azobenzene and the thiol-reactive MTS moiety is the linkage which has the greatest influence on the thermal stability of the compounds. The type of linkage chosen for this site was alkyl, amide, carbamate and urea. Photoisomerization of the crosslinker from the trans to the cis state attached to the test peptide FK-11 caused a decrease of the peptide helix content. The half-life of the cis state at 37 ℃ was 12 hours, 3 minutes, 33 seconds and 10 seconds for the different types of linkages (alkyl, amide, carbamate and urea) and at 25 ℃ 43 hours, 8 minutes, 96 seconds and 26 seconds. Chi, et al (89) used a disubstituted N, N-dialkyl azobenzene derivative in the two peptides FK-11 and JRK-7. The half-life of the cross-linked FK-11 was 76 ms with increased peptide helix content when relaxed from cis to trans. For JRK-7 the half-life of the cis form was 6.5 ms with decreased peptide helix content when relaxed from the cis to the trans form. To cite Pozhidaeva et al (88): "Additionally, a rapid thermal relaxation to the trans form, ensures virtually complete conversion to the trans isomer, important where a complete "off" state is desired for a biochemical switch."
Willner, et al (90) modified the enzyme papain with azobenzene-4-carboxylic acid and the activity of the enzyme was assayed by following the rate of hydrolysis of N-α-benzoyl-DL-arginine-4-nitroanilide hydrochloride (BAPNA). By studying the absorption bands it was concluded that illumination with λ = 320 nm increased the proportion of cis-configuration and illumination with λ > 400 nm increased the proportion of papain with trans configuration, but not to 100%. It is a photostationary equilibrium when the enzyme is illuminated with λ = 320 nm and λ > 400 nm respectively. Five on-off cycles were performed with no detectable decrease in the biocatalytic photoregulative activity. With the same Vmax but higher Km in the Lineweaver-Burk plot for the iso-form of papain it was concluded that the decrease in the enzymatic activity of the cis-form was similar to competitive inhibition. The enzymatic activity of the trans form of papain was 80% of the enzymatic activity of the non-modified papain and the enzymatic activity of the cis-form of papain was 30% of the enzymatic activity of the non-modified papain.
NLS (Nuclear Localization Signal) is a peptide when bound to Kap α directs a protein to the cell nucleus. If an amino acid containing azobenzene is introduced into the NLS the ability of the protein to be transported to the cell nucleus can be switched on and off by light. Azobenzene has been used to construct a synthetic amino acid, mp-Abc, which was designed from another synthetic amino acid, p-Aza, in order to amplify the photoelastic behaviour of p-Aza (91). A library of 30 mutants of the bipartite NLS, a peptide motif which directs the transport of proteins into the nucleus by binding to Kap α, from Xenopus laevis (African clawed frog) was created using parallel, solid phase synthesis and screened in vitro for binding to the nuclear import receptor karyopherin (Kap α) which mediates the nuclear import of cellular proteins. Systematic mutagenesis was performed with mp-Abc introduced into all possible locations within the linker. Of these 30 mutants one had different enough affinities between the cis and trans photoisomers, it was named pKL-1c as it was only the cis isomer which bound to the receptor. pKL-1c bound slightly weaker to the native nucleoplasmin NLS in the cis form but had no detectable binding to the NLS in the trans form. Photoisomerizable amino acids are Pap, p-Aza, mp-ABC and its isomers, PATIC, and three phospho-amino acid analogues typified by Ppp.
A systematic and exhaustive scanning mutagenesis can be used for any peptide-receptor system for which a reliable screen exists. The method requires one or more photoisomerizable amino acids, an efficient synthetic strategy and a rapid screen. NLS is a transferable motif. NLS from one protein and attached to another protein by genetic fusion or chemical cross-linking will direct the other protein into the nucleus. It is possible to ligate synthetic molecules site-specifically to essentially any protein which can be expressed in Escherichia coli.
The azobenzene compound TBA (3,3',5,5'-tetra-tert-butylazobenzene) absorbed to Au (gold) can have its trans to cis and cis to trans isomerizations under the influence of an electric field instead of light, without the tunnelling of electrons. The investigation was carried out in ultrahigh vacuum at a temperature of 5K in a STM (scanning tunnelling microscope) (92). To isomerize cis azobenzene to trans azobenzene energy in the form of light can be substituted with an external force 1250-1650 pN (1 pN = 1 picoNewton = 10-12 kgm/s2) which accomplishes the isomerization by a mechanically activated inversion followed by an ultrafast rotation (93). This shows that light as a necessary prerequisite to achieve isomerizations of azobenzene can be substituted by an electric field and by a mechanical force but what is required is to substitute light by energy transferred from a scintillator which in turn has received energy by absorption of ionizing radiation.
In NEE the physical clearance of the conjugates will be achieved through ordinary routes (liver, kidneys, reticuloendothelial system), the clearance of the function of the conjugates will be achieved by thermal relaxation of the photoswitches (T-type photochromism).
Asymmetric photochemistry. The polarization state of radiation can influence the proportion of right and left enantiomers in a chemical reaction. R-CPL (right circularly polarized light) and L-CPL (left circularly polarized light) can have this effect on a chemical reaction (asymmetric photochemistry = chiral photochemistry) (94). It is believed that UV-CPL (ultraviolet circularly polarized light) is the cause of the predominance of L-forms in the production of amino acids in interstellar space and is the reason that proteins in all living organisms are made of L-amino acids instead of R-amino acids (95).
Applying R-CPL or L-CPL to a chemical reaction can cause an excess of the amount of one product enantiomer over the other. The enantiomeric excess (ee) in a mixture of R and S enantiomers is defined as ee = (CS-CR)/(CS + CR). ee is sometimes called optical or enantiomeric purity. Besides CPL to produce a non-zero ee, enantiodifferentiating photosensitized reactions can be used which implies the use of an optically active sensitizer which through noncovalent interactions on the excited state achieves chirality amplification. Problems associated with asymmetric photoreactions are often low enantiomeric excess and slow response times. To cite Feringa, et al (96): "It is evident from the various systems developed so far that the field of chiroptical molecular switches is still in a premature state."
A combination of light and a magnetic field can give rise to asymmetric photoreactions ("Magnetochiral anisotropy in asymmetric photochemistry") (94). Avalos et al has reviewed the effects of physical fields on chemical reactions (97). These authors use the concept of true and false chirality which is based on the symmetry operation of parity P and time reversal T which according to the authors often is simpler and more intuitive than the invariance properties of the Hamiltonian of a molecule in the presence of an external influence. Physical fields which are considered are magnetic and electric fields, magnetochiral fields, gravitational fields and vortex rotation, polarized photons, electrons and neutrons and other fields including radiofrequency radiation, microwaves and ultrasound.
In NEE there are four kinds of transport: Radiation, blood flow, diffusion in articular cartilage and intracellular transport.
There is a "circulation field" or a "flow field" applied as the blood flows in the arteries, capillaries, canaliculi and veins with the consequence that after the conjugates have been activated their location is dependent on time. If the conjugates for motif number one are to be injected intraarticularly and not intravenously the flow field also depends on the circulation of the fluid present in the articular cavity at the time of the treatment, in addition to diffusion in the intercellular substance of the articular cartilage.
The blood flow in bone in young white female rats has been investigated using a radioisotope dilution technique. In the superior metaphysis of the femur the blood flow was 22 ml/100 g/min, in the marrow 29 ml/100g/min and in the cortex 17 ml/100 g/min (98). The flow through the bone lacunar-canalicular system (LCS) has been studied in 12-16- week-old male mice using fluorescence recovery after photobleaching (FRAP). The peak canalicular fluid velocity in loaded bone was estimated to be 60 μm/s (99).
There is a difference between motif no. 1 and the other three motifs regarding the requirement on the half-life of the active state of the photoswitch which is caused by the expected longer transport time through the intercellular matrix of the articular cartilage compared to the faster transport in the capillaries/canaliculi of bone tissue. The half-life of the active state of the photoswitch in motif no. 1 has to be longer than the half-life of the active state in motifs no. 2-4 which means that it must not enter the systemic circulation through the synovial membrane in the joint capsule.
If the conjugates for motif no. 1 are to be injected intraarticularly there is also the question of any possible flow in the synovial fluid (perhaps the patient moves the hip joint) and the exact localization of the conjugate (in the synovial fluid or in the articular cartilage) when the targeted radiative ON-signal is given. If the conjugate is in the synovial fluid perhaps it will be transported to another part of the articular cartilage where it was not intended and enter the articular cartilage there or be absorbed by the synovial membrane and enter the systemic circulation. If the conjugate is in the articular cartilage perhaps it will diffuse out again and be transported to another part of the articular cartilage or diffuse to a non-intended area.
Some facts about gene control have been compiled from the book Gene Control by David S. Latchman (100):
Chromatin structure. Gene control is performed at the level of chromatin structure, transcription and post-transcription. Most of the genes are organized into a tightly packed 30 nm fibre structure. The nucleosome is the basic unit of the folded DNA consisting of about 200 bp (base pairs) of DNA wrapped around an octamer of histones, a pair each of the four histones H2A, H2B, H3 and H4. Three processes regulating chromatin structure are DNA methylation, histone modifications, particularly acetylation and methylation, and ATP-dependent remodulation of chromatin structure by complexes such as SWI-SNF and NURF. These changes are linked. DNA methylation can stimulate histone changes such as deacetylation and methylation which in turn may regulate SWI-SNF recruitment to the promotor.
Active or potentially active DNA is organized in the beads-on-a-string structure. The 30 nm fibre structure is formed by most of the DNA that is not about to or being transcribed. The demethylation of genes is characteristic of genes which are active or potentially active and associated with a beads-on-a-string structure of the DNA. Dnmt3a and Dnmt3b carry out de novo methylation of unmethylated sites. DNA-methylation can be maintained during DNA-replication and thus stabilize the committed state of the cell. During DNA-replication the cytosine on the other DNA-strand is methylated by the DNA methyltransferase enzyme Dnmt1 if the cytosine on the original DNA strand is methylated. There are a number of different proteins, for example MeCP2, able to bind to methylated CG causing a tightly packed chromatin structure and transcriptional repression.
Hyperacetylation of lysine in histones plays a role in opening the chromatin structure of active or potentially active genes. Methylation can occur for both lysine and arginine amino acids of histones. Methylation of specific arginine residues and of some lysine residues is associated with a more open chromatin structure and transcriptional activation whereas methylation of other lysine residues produces a more tightly packed chromatin structure and transcriptional repression.
Methylation of histone H3 on lysine 9 allows it to be recognized by the protein HP1 (heterochromatin protein 1) which is able to organize the chromatin into a very tight inactive structure characteristic of heterochromatin. Furthermore, HP1 can in turn recruit a histone methyltransferase enzyme, catalysing the lysine 9 methylation of histone H3 in adjacent nucleosomes. Thus, the tightly packed heterochromatin structure produced by HP1 will spread along the DNA producing a large region of tightly packed DNA until the spreading structure encounters a sequence such as an "insulator" which prevents the spread of a particular structure to an adjacent region. The pattern of H3 methylation may be stably inherited by a mechanism similar to the propagation through mitosis of DNA methylation.
The addition of the small protein ubiquitin occurs only for the histones H2A and H2B. About 5-10% of the H2A in a cell exists in this form and such ubiquitination is associated with the repression of gene expression. Ubiquitination of H2B has the opposite effect to the ubiquitination of H2A since it stimulates rather than inhibits gene expression. Ubiquitinated H2A inhibits and ubiquitinated H2B promotes recruitment of the FACT protein which is essential in elongation of the initial RNA transcript.
Lysine residues on histones can also be changed by the addition of a small ubiquitin-related modifier (SUMO) causing transcriptional repression due to the recruitment of enzymes which deacetylate histones causing a more closed chromatin structure.
Phosphorylation targets serine or threonine amino acids in the histone molecule causing a more open chromatin structure allowing transcription to occur. When cells are stimulated to undergo cell division by treatment with growth factors histone H3 is phosphorylated on the serine residue at position 10 in the N-terminus of the protein. These phosphorylated histones are localized to genes which become transcriptionally active following growth factor stimulation, such as c-fos and c-myc genes. Phosphorylation also occurs on histone H1, reducing its ability to interact with the HP1 protein, important in producing the very tight chromatin structure of heterochromatin. Phosphorylation of H1 may be a decisive event in moving from a tightly packed chromatin structure to a more open one.
There is an interaction of different histone modifications with each other, a modification of one amino acid in a histone can promote or inhibit the modification of adjacent amino acids on the same histone and the modification of one histone can affect the modification of another histone. By the concept of a "histone code" is meant the particular pattern of modified histones which can recruit regulatory proteins recognizing the specific pattern instead of a modification at a single site. Specific histone modifications not only influence the modification of other sites in the same or different histones but together with variant histone isoforms can also influence methylation of the DNA.
Small interfering RNAs (siRNAs) can repress gene expression at the level of transcription by directing the formation of a tightly packed chromatin structure. siRNAs are produced by cleavage of a longer double-stranded RNA precursor by the Dicer protein. When the siRNA represses gene transcription it binds to a complex containing an Argonaut protein and is known as the RNA-induced transcriptional silencing (RITS) complex. The siRNA and RITS complexes then bind to target genes resulting in their transcriptional repression. siRNAs play an important role in the formation of the very tightly packed chromatin structure of heterochromatin. They bind to complementary sequences in the target gene and then recruit the HP1 protein which plays an essential role in the formation of heterochromatin. It has the ability to produce inhibitory methylation of histones and to recruit DNA methyltransferases which methylate the DNA on C residues.
The nucleosome is a highly dynamic structure. The DNA is continuously unwrapping from the histone octamer, remaining exposed for a short period and then rewrapping around the histones. Several multi-protein chromatin-remodelling complexes exist in eukaryotic cells, for example the SWI/SNF family and the ISWI family. Each of these complexes contains an ATPase component to generate the energy for the remodelling process which as a result may cause a change of the structure of the nucleosome causing the DNA to be more exposed, cause a displacement of the nucleosome making it move along the DNA or a displacement of the nucleosome so that it is lost from the DNA facilitating the binding of activator molecules to the DNA.
Genomic imprinting may inactivate the maternally or paternally derived gene while the other gene is active, a specific methylation pattern of CG dinucleotides is involved. Similar modifications and changes in chromatin structure are involved to regulate cellular commitment and gene expression in specific cell types as well as X-chromosome inactivation.
Transcriptional control. In the nucleus of all eukaryotes there are RNA polymerase 1, 2 and 3. The genes encoding the 28, 18 and 5.8 S ("S" is the Svedberg unit, a non-SI unit, for sedimentation rate) ribosomal RNAs are transcribed by RNA polymerase 1. Genes capable of encoding a protein and genes for some small nuclear RNAs involved in RNA splicing are transcribed by RNA polymerase 2. RNA polymerase 3 transcribes genes encoding the transfer RNAs and the 5S ribosomal RNA.
Several genes transcribed by RNA polymerase 2 contain an AT-rich sequence found about 30 bases upstream of the transcription start site, the TATA box, which plays a critical role in promoting transcriptional initiation and in positioning the start site of transcription for polymerase 2.
The TATA box acts as the initial DNA target site for the progressive assembly of the basal transcription complex for RNA polymerase 2. Initially, the TATA box is bound by the transcription factor TF11D whose binding is facilitated by the presence of another transcription factor TF11A.
Subsequently, the TF11D-DNA complex is recognized by another transcription factor TF11B. TF11B binds on the opposite side of TF11D to that which is bound by TF11A. TF11B can recruit RNA polymerase 2 itself, in association with another factor, TF11F. Afterwards, two other factors TF11E and TF11H associate with the complex. One component of TF11H has a kinase activity which phosphorylates the C-terminal domain of the largest subunit of RNA polymerase 2, known as RPB1, allowing transcription initiation to occur.
Each of the three polymerases has a similar pattern of recruitment to the DNA with one specific transcription factor binding to a target sequence in the gene promotor followed by binding of one or more other proteins which then recruit the polymerase itself.
TF11D is a multiprotein complex containing TBP (TATA - binding protein). The other components, TBP-associated factors (TAFs), do not bind directly to the TATA box but appear to allow TF11D to respond to stimulation by transcriptional activators.
A subset of RNA polymerase 2 genes does not contain the TATA box but instead an initiator sequence (Inr) located around the transcriptional start site. TBP is an evolutionary ancient transcription factor involved in transcription by all the three RNA polymerases.
Transcription of some genes can occur without TBP instead using a TRF (TBF-related factor) or without both TBF and TRF.
Capping, the addition of a modified G nucleotide to the free 5' end of the nascent DNA transcript, occurs when the RNA transcript is 20-30 bases long and promotes the binding of the pTEF-b kinase protein which phosphorylates the C-terminal repeat of RNA polymerase 2 on serine 2 allowing transcriptional elongation to occur.
The region around or just upstream of the transcriptional start site containing the TATA box and/or the Inr sequence (or the equivalent region of genes when they are absent) is known as the core or basal promotor and serves to recruit the basal transcriptional complex. The core promotor serves as the minimal region which can direct the initiation of transcription. However, even when a TATA box and/or an Inr sequence is present, this produces only a relatively low rate of transcription. This rate of transcription is increased by the presence of upstream promotor elements, located upstream of the core promotor. Together, the core promotor and the upstream promotor elements constitute the promotor, which drives the transcription of the gene.
Binding of a specific protein may result in displacement of a nucleosome allowing easy access to the gene for other transcribing factors. These factors are likely to act by interacting with proteins necessary for transcription such as TBP or RNA polymerase itself.
Enhancers lack promotor activity and are unable to direct transcription themselves but they can dramatically enhance the activity of promotors. The definition of an enhancer is that it can activate a promotor when placed up to several thousand bases from the promotor, it can activate a promotor when placed in either orientation relative to the promotor and an enhancer can activate a promotor when placed upstream or downstream of the transcribed region or within an intervening sequence which is removed from the DNA by splicing. Hence the typical eukaryotic gene will contain enhancer elements as well as core and upstream promotor elements.
In many cases the tissue-specific expression of a gene will be determined both by the enhancer element and sequences adjacent to the promotor.
The array of different regulatory proteins which assemble on such an enhancer has been called an "enhancerosome". Enhancers can activate gene expression by a change in chromatin structure leading to nucleosome displacement or by direct interaction with the proteins of the transcriptional apparatus via looping or bundling of the DNA.
Silencers can act on distant promotors when present in either orientation and have an inhibitory effect on gene expression. As with enhancers they act at the level of chromatin structure by recruiting factors which direct the tight packing of adjacent DNA or by binding a protein which then directly inhibits transcription by interacting with RNA polymerases and their associated factors.
Protein motifs of transcription factors which bind to DNA include the helix-turn-helix domain, the zinc finger, the multi-cysteine zinc finger in nuclear receptors and the leucine zipper which facilitates dimerization of the protein allowing the adjacent region of the protein to bind to DNA. Dimerization of transcription factors can produce new specificities of DNA-binding resulting in both stimulation and inhibition of transcription.
Protein domains in activators which exert the activating function are the acidic region, the glutamine-rich region and the proline-rich region. Activators can interact with a variety of different targets with the basal transcriptional complex. A co-activator does not bind to DNA directly but mediates the effect of DNA-bound activators.
Repressors can act indirectly by inhibiting the positive effect of activators and directly by inhibiting the assembly or activity of the basal transcription complex. A key target for factors which regulate transcriptional elongation is the phosphorylation of the c-terminal domain of RNA polymerase 2.
Post-transcriptional control. Before transcription is completed the 5' end of the mRNA is modified by "capping", the addition of a guanine residue which is not encoded by the DNA. A methyl group is added to the guanine producing 7-methyl-guanine. In higher eukaryotes additional methyl residues may be added to the first and sometimes also the second of the two transcribed nucleotides immediately following the 7-methyl guanine.
In eukaryotes the AUG initiation codon may be located several hundred bases away from the 5' end of the RNA. Following binding at the cap, the 40S subunit of the ribosome migrates along the mRNA until it encounters the appropriate AUG initiation codon. At this point the large (60S) ribosomal subunit binds and transcription begins.
Translation is not initiated at the first AUG which it encounters by the small ribosomal subunit. The AUG triplet must be set within the appropriate consensus sequence which is related to GCCA/GCCAUGG. The rules which determine whether a particular AUG codon will allow the ribosome to initiate transcription are known as Kozak's rules.
As the first step of translation, the cap on the mRNA is recognized by the translation initiation factor e1F4E. This results in the recruitment of other translation factors and of the small ribosomal subunit itself. The cap structure also protects the 5' end of the mRNA from attack by exonuclease enzymes. This protection from degradation is achieved by the binding to the cap of the cap-binding complex (CBC) which also facilitates the transport of the mRNA to the cytoplasm. In the cytoplasm CBC is displaced from the cap by e1F4E allowing the mRNA to be translated into protein. Once capping has occurred the pTEF-b kinase is recruited and it phosphorylates RNA polymerase 2 so that transcription continues and the full transcript is produced.
After transcription the 3' end is removed and up to 200 adenosine residues are added (polyadenylation), the process protects the mRNA from being degraded by exonucleases and is believed to regulate the efficiency by which an mRNA is translated.
Virtually all eukaryotic introns for genes transcribed by polymerase 2 begin by the bases GU and end with the bases AG. A small number begin with the sequence AU and end with AC. RNA splicing takes place in the spliceosome consisting of five different RNAs and over a hundred proteins. The RNA components of the spliceosome are small RNA molecules known as the U RNAs because they are rich in uridine residues. Each of these U RNAs has a specific role in the splicing process and each of them is associated with specific proteins forming small nuclear ribonucleoprotein particles (snRNP) which consist of a U RNA with its associated proteins.
The spliceosome also contains other proteins which are not directly associated with the U RNAs. SR-proteins (rich in serine and arginine residues) are believed to serve both in recruiting the snRNPs to the RNA to be spliced and in determining which splice sites are joined to one another. It appears that the SR proteins bind to sequences within the exons known as exon-splicing enhancers (ESEs) and ensure that the exon is included in the final spliced RNA rather than being spliced out.
The SR proteins also have an important role in the process known as alternative splicing in which different combinations of exons can be joined to one another in different situations. "Trans-splicing" occurs between exons from different mRNAs producing a chimeric mRNA.
Transcription, capping, polyadenylation and splicing are tightly coupled together within the nucleus and the factors involved in different post-transcriptional processes interact with one another.
The transport of the fully processed mRNA through the nuclear pore involves it becoming associated with the RNA exporter complex (REC) which consists of two proteins, TAP (also known as NXF1) and p10C (also known as NXT1). The mRNAs encoding functionally linked proteins can be exported together, facilitating their translation in parallel and the subsequent functional association of their corresponding proteins.
In eukaryotes translation is initiated by the binding of the eukaryotic initiation factor (eIF), eIF4E, to the cap structure at the 5' end of the mRNA, replacing the CBC. Subsequently, other eIF factors, such as eIF4G and eIF4A/B bind to the 5' end of the RNA. Together eIF4A, eIF4E, and eIF4G form a complex which is known as eIF4F. The binding of the various components of the eIF4F is followed by the binding of a complex consisting of the small 40S ribosomal subunit, a transfer RNA (tRNA) molecule which carries the amino acid methionine, and the initiation factor eIF2. Then the 40S subunit migrates down the mRNA until it finds an AUG initiation sequence in the mRNA which is located in the appropriate context for the initiation of the translation. Ultimately, the moving ribosome encounters one of the three stop codons (UAA, UAG or UGA) which are not recognized by a specific tRNA and a release factor (CRF1) catalyses the release of the completed polypeptide from the ribosome.
An incorrectly processed mRNA will be degraded in the nucleus by a multiprotein complex known as the exosome which contains a 3' to 5' exonuclease. Introns are degraded in the same way.
Degradation of functional mRNAs in the cytoplasm begins with de-adenylation, removing of the polyA tail of the mRNA. The degradation of mRNA in the cytoplasm takes place in small granular structures known as P-bodies.
RNA splicing can be regulated. A single gene which is transcribed in several different tissues can be spliced in different ways in the different cell types. Over 90% of human genes with multiple exons are alternatively spliced.
In situations where the 5' end of the transcript is different, two alternative primary transcripts are produced by transcription from different promotor elements and they are processed dissimilarly. In several situations differential splicing is controlled simply by the presence or absence of a particular exon in the primary transcript. The variation in RNA splicing is secondary to the primary choice involving the selection of different promotors in the different tissues.
Splicing factors can act negatively to inhibit the use of a particular splice site or positively to promote the use of a particular splice site. As well as responding to the presence or absence of a specific factor, specific RNA sequences can also regulate the pattern of alternative splicing in response to cellular signalling pathways.
Alternative splicing involves the interaction of a number of factors with sequences within the mRNA itself and constitutively expressed or tissue-specific protein factors. Each splice site within the RNA will have a particular strength depending on several factors. The strength of a splice site will also depend on the presence or absence of ESEs (exon-specific enhancers). There is also an effect of position, i.e. whether the splicing event involves a proximal or distal downstream exon.
Splicing is closely linked to transcription itself. The use of alternative promotors for transcription of a particular gene can influence the pattern of alternative splicing by producing RNAs which fold in different ways or by recruiting different splicing complexes.
Transcriptional elongation can influence which alternative splicing event occurs. When an upstream 3' splice site is weaker than a downstream one, a low rate of transcriptional elongation will favour the use of the weaker site since it can be used before the downstream site has even been transcribed. In contrast, with a faster rate of transcriptional elongation, both splice sites will be present in the RNA transcript which is being spliced, resulting in the stronger splice site being used. Alternative splicing can be used to control the level of a particular protein.
RNA editing involves a change from a C to a U residue and a change from an A (Adenine) to an I (Inosine) residue that is read as a guanine residue by the translation apparatus. A-to-I editing can target protein-coding mRNAs to alter the encoded protein or the splicing pattern.
Specific sequences in the mRNA are involved in its stability. Changes in stability of a particular mRNA are very often accompanied by parallel alterations in the transcription rate of the corresponding gene.
Translational control may cause changes in the translation of many RNA species and may also operate on individual RNAs in a particular cell type. It can act via modification in the cellular translational apparatus affecting the efficiency of translation of particular RNAs. Alternatively, it could involve proteins which recognize specific sequences in the RNA itself and which affect translation.
Regulation of gene expression can also be achieved by very small RNA molecules of between 20 and 30 bases in length. These small RNAs can produce their inhibitory effect at the level of transcription by modulating chromatin structure but mostly they achieve their effect post-transcriptionally either by promoting mRNA degradation or by blocking translation.
If there is a perfect base-pair match between the small RNA and its target mRNA, as normally occurs with siRNA and in some miRNA cases, the mRNA will be degraded. The siRNA or miRNA is not cut in this process but remains intact. It can therefore bind to other copies of its target mRNA and induce their degradation making the process of gene repression by small RNAs highly efficient.
In most cases involving miRNAs, the miRNA will not have perfect complementarity to its target sequence, a single miRNA then can hybridize to many different mRNAs and by reason of that repress a number of different genes. A significant number of miRNA targets are themselves regulatory proteins such as transcription factors and regulators of alternative splicing.
Mills (101) has outlined requirements on the optimal inducible gene expression system. Optogenetics is mainly tested in the nervous system (102).
Cys2His2 zinc finger proteins bind to 3-4 base pairs in the DNA. By combining two or more zinc fingers almost every site on the DNA can be targeted. To produce a zinc finger which binds to a specific site on the DNA the phage display method is used, up to 109 different sequences can be tested in each selection. Selections are based directly on the affinity and specificity. By adding other domains to the zinc finger protein activation or repression of transcription of a specific gene can be achieved (103).
By combining a Cys2His2 zinc finger protein with the GIGANTEA protein and the LOV (light-oxygen-voltage) domain of FKF1 in Arabidopsis thaliana (a small plant) a blue light inducible spatiotemporal control of gene activation in human cells has been achieved (104).
Zinc finger proteins have been used to achieve drug-inducible regulation of transcription in response to two ligands, ethyl-4-hydroxy benzoate and propyl-4-hydroxy benzoate in a dose-dependent manner, in human cells (HeLa-cells) (105).
There are systems for spatiotemporal control of gene expression in mammalian cells that do not use zinc finger proteins. The LightOn system uses a single chimerical protein (GAVPO) that can homodimerize and bind to promotors upon exposure to blue light, activating transcription of a target gene (106). GAVPO is an optimized light switchable transactivator consisting of three parts: Gal4(1-65), VIVID, and p65. Gal4(1-65) is the DNA-binding domain of the regulatory protein Gal4 from yeast that can specifically recognize and bind to an UASG element (UAS = upstream activating sequence). VIVID is a light-oxygen-voltage (LOV) domain containing protein which can form a homodimer upon exposure to blue light. The p65 activation domain from NK-KB is an efficient human activator, it can stimulate transcription from proximal promotor and remote enhancer positions.
Light-inducible transcriptional effectors (LITEs) are optogenetic two-hybrid systems integrating the TALE DNA-binding domain with the light-sensitive cryptochrome 2 protein and its interacting partner C1B1 from Arabidopsis thaliana. LITEs can be packaged into viral vectors and they can be used for control of mammalian transcription and epigenetic status (control of histone modifications) (107).
A red/far-red light responsive toggle switch to control gene expression in mammalian cells has been constructed of the photoreceptor phytochrome B (PhyB) and the phytochrome-interacting factor 6 (PIF6) of Arabidopsis thaliana. Transfection with plasmids were used (108).
Azobenzene has been used to control gene activation by light (109).
Gene therapy is based on one of two principles, "transductional targeting" which is the delivery of genes to specific cells and "transcriptional targeting" which is the use of promotors causing the expression of specific genes in targeted cells (110). Transductional targeting can encompass the insertion of the gene(s) into the genome of the host cell which means that the gene(s) is replicated during mitosis or remain outside of the genome in the nucleus of the host cell as an "episome" and owing to that is not replicated during mitosis of the cell.
Clinical trials with gene therapy has been instituted against cancer, cardiovascular disease, neurological disease, infectious disease, inflammation diseases and against genetic diseases such as haemophilia, cystic fibrosis, SCID and muscular dystrophy.
The vectors have mostly been viral in origin including modified adenoviruses, adenoassociated viruses, retroviruses, poxviruses and herpes simplex viruses.
Adeno-associated virus (AAV) has been used for prolonged gene expression in different tissues, eye, brain, liver and lung. AAV belongs to the parvovirus family, is one of the smallest DNA animal viruses, the virion is about 25 nm in diameter. AAV is a "dependovirus", it requires the simultaneous infection with another virus such as adenovirus or herpes simplex virus in order to achieve productive infection in cell culture. Vp3 is the part of the virus which is used to recognize receptors on cells which the virus can infect. By substituting replication and capsid genes with a promoter and gene of interest rAAV's can be produced. Targeting of cells has been accomplished by a bispecific antibody. Concerning targeting through modification of the capsid there are different requirements. The targeting ligand must be placed in the capsid in such a way that the packaging of DNA is unaffected and the ligand is accessible on the surface of the virus. The vector must be altered in order to prevent it from binding to its native cellular receptors. Because it is difficult to know the secondary structure of the ligand after it has been placed on the capsid it is recommended to use a small ligand which is independent of structure and which does not destabilize the capsid. The ligand must target a receptor which permits internalization leading to transport of the virus to the cell nucleus. A new technique in producing targeting ligands involves the construction of a peptide library in a three-step process. Each peptide consists of seven amino acids in a random order located at the surface of the capsid at amino acid no. 588. The peptides are encoded by the packaged DNA. Each library has 1.1 x 108 clones. A great number of cell lines can be screened in order to identify library clones which can target them. To add an additional level of safety tissue-specific promotors are recommended. Prolonged gene expression can be hindered by humoral and cell-mediated immune responses.
"Pseudotyping" denotes the substitution of a viral attachment protein (VAP) with the VAP of another compatible virus. Because of the connection between binding to a cell and fusion with the cell it is difficult to alter binding specifically without decreasing fusion or packaging ability of the vector. As simple retroviruses cannot infect post-mitotic cells, efforts have been made in order to engineer complex viruses, lentiviruses and foamy viruses which have the ability to infect nondividing cells. "Inverse targeting" in retroviral vectors means that high affinity ligands on the envelope are blocked from binding to the receptors on the cell because the virus sequesters the receptor. Targeting development with library and directed evolution simultaneously screens for the combination of binding and entry properties and can be applied to cells which are not characterized with any detail.
Lentiviruses can have long-term expression in different kinds of stem cells and may be less amenable to silencing, they are mutagenic as the host genome is irreversibly changed by integration into the host genome. To reduce risk with this vector self-inactivating vectors, coexpression of a suicide gene and inducible vectors which change expression due to the presence or absence of an exogenous regulating small molecule have been proposed. Apart from antibodies and lymphocytes cells can block viruses by transcriptional silencing by condensation, methylation, binding of methyl-CpG-binding protein 2 to methylated promotors or recruitment of histone deacetylators.
Lipid- and polymer-based gene transfer is mediated by cationic lipids (lipoplex), cationic polymers (polyplex) or lipid-polymer hybrids (lipopolyplex) (111). Nuclear uptake of the DNA and its expression is lower compared to the use of viral vectors, it is tried to mimic the tools viruses have for its transfection, to construct "synthetic viruses". The gene therapy also includes RNA interference (RNAi), discovered in 1998, based on reversible silencing of specific genes causing disease by delivering short interfering RNA (siRNA) and micro-RNA (miRNA) to the target cells. In a lipoplex the positively charged hydrophilic head group condenses with the negatively charged DNA and the hydrophobic tail forms micellar or bilayer structures around the DNA, protecting it from nucleases. Cellular uptake is facilitated by the electrostatic interaction between the negatively charged cellular membrane and the positively charged head groups. PEG (polyethylene glycol) is added ("PEGylation") to the surface in order to increase circulation time (protection from the immune system, "stealth technology"). PEI, polyethylenimine and PLL, poly(L-lysine) were two of the earliest cationic polymers. Second generation polymers include a poly[(2-dimethylamino)ethyl methacrylate] (pDMAEMA), poly-arginine containing proteins, poly(beta-amino ester), polylactic-co-glycolic acid (PLGA)-based nanoparticles, carbohydrate based polymers such as heparin and dextran, and dendrimers.
Hybrid lipid-polymer-based nanoparticles (lipopolyplexes) usually consist of a polycation-DNA core with an outer shell of lipids.
Certain short peptides can pass through the cell membrane and bring large biologically active molecules. These short peptides are called cell-penetrating peptides (CPPs), membrane translocating sequences, "Trojan peptides" or protein transduction domains (PTDs). They consist of 7-30 amino acids and have a net positive charge. One example is R8 (octaarginine).
Active targeting is performed by targeting ligands which stabilize the carrier at the outside of the cell or trigger receptor-mediated endocytosis and internalization, and passive targeting by altering biophysical qualities such as size and charge.
Polyethylenimines (PEIs) are effective and versatile agents for nucleic acid delivery in vitro and in vivo. The high transfection efficiency is believed to depend on the "proton sponge" effect, PEI buffer the endosomes which leads to the accumulation of protons followed by passiv influx of chloride ions, osmosis and swelling which leads to disruption of the endosomes so that their contents get out into the cytosol. This "proton sponge effect" has been disputed. The amino groups also make modifications such as addition of targeting groups and PEGylation possible and can interact effectively with DNA.
"Bioresponsive" polymers can vary their structure according to their environment with regard to pH, redox potential and enzymatic activities. ("redox" is short for "reduction-oxidation", oxidation is the gaining of electrons and reduction is the giving away of electrons. This can be compared with "pH" which is the negative 10-logarithm of the concentration of protons (hydronium ions), "pH" is related to protons and "redox" is related to electrons).
The redox potential is mainly regulated by GSH (glutathione), thioredoxin (Trx) and cysteine (Cys). The disulphide bond (-SS-) in proteins can be cleaved in the reductive cytosol but is stable in the less reductive extracellular fluid. Thiol groups (two thiol groups, -SH, can together form a disulphide linkage) and disulphide linkages in polymers make the polymers responsive to changes in the redox potential. The concentration of GSH in the blood is about 1-10 μM and in the cytosol 1-10 mM causing the cytosol to be more reducing than the blood. Proliferating cells have the lowest redox potential followed by differentiating, apoptotic and necrotic cells.
pH is around 7.4 in the blood and around 7.2 in the cytosol and even lower in the endosome and lysosome. Proliferating cells have a cytosolic pH up to 7.4. Acid-labile linkers such as imine, orthoester, acetal/ketal and maleic acid amide (MAA) can be inserted into the polycation main or side chain to make it biodegradable at a lower pH.
Enzymatic substrates such as peptide linkages, nucleotide linkages and ester linkages have been inserted to make polymers and polyplexes change their structure in response to the changing environment's content of the enzymes acting on these linkages. A biosignal which can be used to release siRNA into the cytosol is ATP (adenosine triphosphate) which has a cytosolic concentration of 1-10 mM and an extracellular concentration of about 0.4 mM.
PEIs can be cytotoxic through different modes of cell death pathways. Apoptosis is a regulated mode of cell death which is used in embryogenesis and development of organs. Apoptosis can be brought about by the extrinsic pathway and the intrinsic/mitochondrial pathway. Both mechanisms consist of an activation phase and an execution phase. The extrinsic pathway is triggered by an external death signal such as binding to a cell surface receptor of tumour necrosis factor-α (TNF-α), Fas ligand (FasL) or TNF ligand super family member 10 (TRAIL). Caspases are active in both the extrinsic and the intrinsic/mitochondrial pathways.
The intrinsic/mitochondrial apoptotic pathway causes the release of cytochrome c from the mitochondria in response to the BcL-2 protein family which increases the permeability of the outer mitochondrial membrane.
PEI decreases the activity of the mitochondrial OXPHOS (oxidative phosphorylation) leading to reduced ATP-production and can cause the release of cytochrome c from mitochondria leading to the activation of pro-apoptotic caspases and programmed cell death.
MEND particles have a lipid envelope with an octaarginine peptide and a DNA core at the centre (112). The octaarginine causes macropinocytosis avoiding degradation in the lysosome. The MEND particles have a diameter of 330 nm (The classical clathrin-mediated endocytosis has endosomes with an upper limit of the diameter of about 150 nm). Transfection with MEND with a luciferase expression plasmid in HeLa cells and A549 cells (both are dividing cells) had the same efficiency as adenovirus mediated transfection and the cytotoxicity was lower. Application on the skin of 4-week-old ICR mice with MEND with constitutively active bone morphogenetic protein (BMP) type 1A receptor (caBmpr1a) resulted in significant influence on in vivo hair growth.
A tetra-lamellar Multifunctional Envelope-type Nano Device (T-MEND) has been used to deliver DNA to the nucleus of non-dividing cells (JAWS 2 cells derived from murine dendritic cells) (113). T-MEND has a core of DNA/polycation surrounded by nucleus-fusogenic lipid which itself is surrounded by endosome-fusogenic lipid. The outer endosome-fusogenic lipid is marked with R8 (the peptide octaarginine), which elicits macropinocytosis at the cell membrane and is shed inside the cell, escaping degradation in the lysosome, after which R8 causes fusion with the nucleus, shedding the inner nucleus-fusogenic membrane, delivering the DNA to the nucleus where it is transcribed. The size of the T-MEND particles was measured by dynamic light scattering, the average value of the diameter was about 160 nm. The route to the nucleus is thus independent of the nuclear pore complex (NPC), "NPC-independent pathway".
Gene therapy in orthopaedics was reviewed by Ulrich-Vinter in 2007 (114).
Grossin, et al (115) injected the plasmid pcDNA 3.1 containing the cytomegalovirus promotor inserted upstream of the coding sequence of the reporter gene GFP (green fluorescent protein) into knee joints of rats. To enhance the transport of the plasmid into the articular cartilage electric pulses were used, 8 pulses of 20 ms at a repetition frequency of 1 Hz with electrical field strength of 250 V/cm. 2 electrodes parallel to the patella were used (electroporation (EP), transitory destabilization of the cell membrane, transport of negatively charged DNA in an electric field). The GFP expressing chondrocytes were located heterogeneously from the superficial layer of the articular cartilage to the deep layer. 48 hours after the EP >65% of the patellar chondrocytes were positively stained with anti GFP-antibody. After 48 hours the percentage of GFP-stained chondrocytes decreased to about 30% for the study period of 2 months. After 1 week the stained cells were hypertrophic chondrocytes mainly in the deep zone, a distribution seen also at 1 and 2 months. In situ hybridization demonstrated persistence of plasmid DNA in the superficial and middle zones at 2 months, suggesting the transgene was silenced but still present.
Grossin, et al (116) injected the plasmid pcDNA3.1/CT-GFP-TOPO vector containing the cytoprotective HSP70 molecule in rat knees to study its effect against osteoarthritis induced by MIA (mono-iodoacetate). The same method of augmenting the transport of the gene to the chondrocytes was used, electroporation (EP), by the application of two parallel electrodes, 12.5 mm apart, parallel to the articular surface of the patella. MIA toxicity measured as LDH-release (LDH = lactase dehydrogenase) or the reduction of tetrazolium salt was lesser when the HSP70 containing vector had been administrated. 48 hours after gene delivery 50% of the chondrocytes were positively stained with GFP antibodies in all areas of the cartilage, the sustained expression was monitored for 3 months, mainly in the deep layer (20-30% positive cells).
Electroporation cannot be used in NEE. In the above works electrodes were parallel to patella which in essence has a flat geometry. The hip joint is not flat. A conclusion drawn from the two above articles is that a method for delivering a conjugate into the chondrocytes of the articular cartilage must account for the percentage of cells which have incorporated the conjugate and whether the percentage varies with the depth of the tissue and how the promotor works with time, if it has been "silenced" by a naturally occurring immunologic mechanism or not.
Consulted literature is Gene Therapy for cartilage and Bone Tissue Engineering by Yu-Chen Hu (117).
Direct vector injection may cause inflammatory response and it is difficult to avoid transgene expression in non-intended nearby tissues. Viruses that have been used are retrovirus/lentivirus, adenovirus, adeno-associated virus (AAV) and baculovirus (117).
Retrovirus contains 2 identical RNA molecules which are reversely transcribed to complementary DNA and integrated into the host genome, such an integration into the host genome is a risk, it could cause cancer. The virus transduces only proliferating cells and because the virus cannot penetrate the extracellular matrix of cartilage it is more suitable for ex vivo transfection. It has a low load carrying ability, about 8 kb. Lentivirus, which belongs to the retrovirus family, can transfect non-dividing cells (117).
Adenovirus can transfect dividing and non-dividing cells and can carry about 8 kb foreign genes. The genome of the virus does not integrate with high efficiency but it remains episomal (outside of the host DNA-molecule), i.e. it is not replicated during cell division so the therapeutic effect becomes less and less in a dividing cell population. The expression is transient, a few weeks, because of cellular immune response against expression of viral proteins inside cells. To reduce the immune response the "gutless" vector has been produced which only contains the viral terminal repeats and the packaging sequences, they are more difficult to produce. Preexisting immunity against adenovirus may be solved by using another serotype of the virus (117).
Adenoassociated virus (AAV) is a parvovirus which needs another virus such as adenovirus or herpes simplex virus for its DNA-replication. AAV alone does not cause serious host immune reactions but many people have neutralizing antibodies against the virus. The virus can have long-term transgene expression in dividing and non-dividing cells (117).
Baculovirus is a diverse group of DNA-viruses able to infect more than 500 insect species. The virus does not replicate and is not toxic inside the transduced mammalian cells. Baculoviral DNA degrades inside the cells with time. Unless selective pressure is applied there is no evidence of integration of baculoviral DNA into the host chromosome. The cloning capacity is 38 kb but a drawback is a short transgene expression of less than 7 days because of its non-replicating nature. To make the expression longer attempts have been made to incorporate AAV inverted terminal repeats or Sleeping Beauty transposon into baculovirus vectors. There have also been constructed hybrid baculovirus vectors which give the transgene an episomal location (117).
Gene therapy for bone tissue engineering. In most of the studies with direct injection the most widely used vectors have been adenoviruses and the genes delivered have been BMP-2, BMP-6, BMP-7 or BMP-9. Direct injection of adenovirus expressing BMP-2 triggers the ossification of segmental bone defects of the femur of rabbits and rats. The new bone which forms has a lower structural organization and strength than the original bone. Direct injection of a retrovirus expressing Cox-2 (= cyclogenase 2, an enzyme that promotes production of prostaglandins promoting angiogenesis and bone formation) into a rat femoral fracture causes bone union of the fracture. Direct injection of adenovirus expressing VEGF into the femur head necrotic regions of rabbits promotes bone formation and re-vascularization in the subchondral necrotic region of the femoral head. Lentivirus vectors expressing small interfering RNA (siRNA) against hypoxia-inducible factor 1α (HIF-1α) and Runt-related transcription factor 2 (RunX2) are developed. The transcription factor HIF increases VEGF gene expression and is associated with coupled regulation of angiogenesis and osteogenesis. RunX2 is a transcription factor associated with osteoblast formation. In the general case, direct injection into a location near a joint may cause ossification of cartilaginous and ligamentous tissues (117).
Gene therapy for cartilage tissue engineering. Growth factors which have been used for chondrogenesis are insulin-like growth factor 1 (IGF-1), bone morphogenetic proteins (BMPs) such as BMP-2, BMP-4 and BMP-6, transforming growth factors (TGF) including TGF- β1, TGF- β2 and TGF- β3, growth and differentiating factor-5 (GDF5). Combinations of BMP and TGF-β have been used for various cell types with chondrogenic potential. The sex-determining region Y box gene 9 (SOX-9) is a transcription factor which can activate chondrocyte specific enhancer elements in the col2a1, col9a1, col11a2 and aggregan genes. SOX-9 is a "master regulator" of the chondrocyte phenotype and SOX-9 is expressed in all chondroprogenitor cells, predominantly in mesenchymal condensations and cartilage. SOX-5 and SOX-6 are also needed for chondrogenesis. Intra-articular injection of AAV (adenoassociated virus), diameter 20 nm, is capable of transducing chondrocytes in vivo and at the same time synoviocytes (120). Delivery of an adenovirus expressing IGF-1 to normal and arthritic rabbit knees is able to increase proteoglycan synthesis in articular cartilage without adverse effects (117).
Gene products might cause negative effects in non-target cells and inflammatory reactions. The dense matrix surrounding chondrocytes is a barrier to in vivo delivery to chondrocytes by almost all vectors. It is often difficult to achieve long-term expression in animal models because of persisting antibodies against AAV or immune response against heterologous transgene products and viral proteins (117).
Comparison with NEE. A model system to test gene therapy in bone tissue engineering is a defect in a long bone in an experimental animal. This is not the case in NEE. In NEE there is no fracture with direct access to the capillaries and the formation of a hematoma. With respect to bone tissue the interest has been directed to osteoblastic activity (corresponding to elimination of deficit volume), not to osteoclastic activity (corresponding to elimination of redundant volume). The direct injection in animal models is in NEE substituted with an intravenous or possibly an intraarticular injection.
If the first step is represented by tissue engineering (119) and the second step is represented by gene therapy in tissue engineering (117) the third step is, besides overcoming the senescence of chondrocytes, remote control of gene therapy in tissue engineering. It is necessary to have remote control (through targeted beams of high-frequency radiation, scintillators and photoswitches, how else?) in order to control the elimination of deficit and redundant volume. Tissue engineering - gene therapy in tissue engineering - remote control of gene therapy in tissue engineering. NEE substitutes the intrinsic guiding system of morphogenesis with an external guiding system, remote control. But, as has been stated earlier, to try to create a substitute for the natural morphogenesis which will function in the adult patient is to have high ambitions.
The intercellular matrix of articular cartilage is too dense for gene therapy to be performed successfully. Therefore, something with the origin outside the cartilage has been tried, an electric field, electroporation, to increase the force with which the genetic material used for the gene therapy can traverse the intercellular matrix and into the chondrocytes.
A complementary approach would be to address the density of articular cartilage itself. In the general case, if matter is to dense for a substance to pass it then the breakage of bonds within the matter in order to increase the distance between the molecules of the matter would allow the substance to traverse it. The problem is then to reverse the process, i.e. to re-create the chemical bonds which earlier have been broken.
To translate this to gene therapy in articular cartilage one realizes that it is necessary to avoid the escape of the chondrocytes from the chondrons and that proteoglycans and other molecules escape from the collagen network. It will be necessary to bring the separated molecular ends together in order to make it possible for the chemical bonds to be formed again, through the addition of enzymes with a reversed action compared to the enzymes (naturally occurring or synthetic) which broke the chemical bonds.
To develop a theory which chemical bounds in articular cartilage should be broken for gene therapy to be possible where the process is reversible leaving no permanent damage to the articular cartilage seems to be an impossible task.
The "standard model" to create a new enzyme for a reaction where the enzyme does not exist in nature deals with the construction of an active site where functional groups of a protein are located in order to stabilize the transition state and to prevent access of the solvent. Laboratory-directed evolution (LDE) is used to improve the active site through induced mutagenesis ("exploration of sequence space") and screening of catalysis (120). Apart from the standard model which focuses on the active site of the synthetic enzyme there are complementary principles used to construct synthetic enzymes which focus on the whole of the enzyme including complete de novo design, entropic effects on activation free energy, dynamical correlations, minimizing the reorganizing energy and electric field optimization (120). Computational chemistry (quantum mechanics applied to chemistry) and molecular modelling are used when constructing synthetic enzymes. An introduction to these two subjects has been written by, among others, A. R. Leach (121), chapters 1-7 in Physical Chemistry (53) give an introduction to computational chemistry.
Artificial enzymes may be viewed as an example of "biomimetic chemistry". To cite R. Breslow (122): "I have coined the term "Biomimetic chemistry" to describe novel chemistry that is inspired by that done in living systems. In that sense modern aviation is biomimetic". With varying success there has been constructed enzymes that use thiamine phosphate as a coenzyme, mimics of enzymes that use pyridoxal phosphate as coenzymes, artificial hydrolytic enzymes including chymotrypsin mimics, metalloenzyme mimics, artificial ribonucleases and artificial enolases and aldolases. There has also been constructed cytochrome P-450 mimics and mimics of vitamin B6-dependent enzymes. Synthetic catalytic domains added to synthetic polymers have elevated catalytic effects on hydrolytic reactions, decarboxylation, Schiff base hydrolysis, aromatic nucleophilic substitution and oxidation. Some of these synthetic polymers can function as peptidases and nucleases. A stable analogue of the transition state of a chemical reaction can be used as a hapten to cause an antibody to show catalytic activity.
Nanoparticles in the form of carbon variants, metal-based nanomaterials, metal oxide-based nanomaterials and other nanomaterials have enzyme-like qualities ("nanozymes"), mainly as regards redox reactions such as peroxidase, oxidase, catalase and superoxide dismutase, and also hydrolytic reactions such as nucleases and esterases (123).
Theoretical considerations concerning the construction of ionizing-radiation-responsive compositions can be found in US patent US5770581 "Gene transcription and ionizing radiation: methods and compositions." (124). The structure of such a composition is according to the patent a synthetic DNA molecule which consists of a radiation responsive enhancer-promotor operatively linked to an encoding region which encodes at least one polypeptide and the encoding region is operatively linked to a transcription terminating region. The radiation-responsive enhancer promotor comprises a CArG domain of an Egr-1 promotor, a TNF-α or a c-Jun promotor. In the composition there should be a sequence encoding a nuclear localization signal.
Ionizing radiation induces expression of the Egr-1 (early growth response 1) gene which encodes a 533-amino acid residue nuclear phosphoprotein with a Cys.sub.2-His.sub.2 zinc finger domain which is partly homologous to the corresponding domain in the Wilms' tumour susceptibility gene. The sequence in the Egr-1 gene which is sensitive to ionizing radiation is a region containing six serum response or CC(A+T-rich)GG (CArG) motifs (125) which are activated by reactive oxygen intermediates (ROIs) (126).
Ionizing radiation also activates the c-Jun/c-fos gene families which encode transcription factors as well as activate the gene encoding TNF-α in certain human sarcoma cells.
The composition also could encompass an encoding region for a polypeptide having radioprotective activity in normal cells. Examples of such polypeptides are interleukin-1, tumour necrosis factor, a tissue growth factor such as hematopoietic growth factor, a hepatocyte growth factor, a kidney growth factor, an endothelial growth factor or a vascular smooth muscle growth factor, interleukin-6, a free radical scavenger or a tissue growth factor receptor. A hematopoietic growth factor could be a colony stimulating factor such as GM-CSF, G-CSF, M-CSF or interleukin-3. An endothelial growth factor is basic growth factor. A vascular smooth muscle growth factor is platelet derived growth factor (PDGF). A free radical scavenger is manganese superoxide dismutase (MnSOD).
The composition also could have an encoding region for a polypeptide with the ability to catalyse the conversion of a pro-drug to a drug or to sensitize a cell to a therapeutic agent.
The expression "operatively linked in frame" signifies that an open reading frame exists between the encoding sequences, they are connected to each other in order to fulfil this requirement.
A nuclear localization sequence permits the encoded transcription factor to enter the nucleus and to interact with DNA in the nucleus. An example of a nuclear localization signal is derived from Simian Virus 40 (SV40) large T-antigen. The composition has a transcription-terminating site required for polyadenylation of transcribed messenger RNA. An example of a transcription-terminating region is the region of nucleotides 1503 to about 2157 of the human growth hormone.
The concept of "effective expression-inducing dose of ionizing radiation" is the dose of ionizing radiation needed to stimulate or turn on a radiation responsive enhancer-promotor. The necessary dose of ionizing radiation depends among other things on the nature of the cell and obviously should be less than the dose which causes cell damage or cell death directly.
The patent calculates with a dose of ionizing radiation between 2 to about 20 Gray (Gy) administrated at a rate of 0.5 - 2.0 Gy/minute. This figure could be compared to those in table 8.4 on page 123 in (62) showing doses and degree of ARS (Acute Radiation Syndrome) related to whole body exposure. 1 - 2 Gy gives mild ARS and >8 Gy is lethal. The figure 2 to about 20 Gy also could be compared to table 16.2 on page 228 in the same book which for example shows that the absorbed dose to the lungs in a chest X-ray (posteroanterior and lateral) is 0.19 mGy. 2 to 20 Gy compared to 0.19 mGy is 2/(0.19 x 10-3) - 20/(0.19 x 10-3) = 10500 - 105000 higher. Further theory about these compositions can be found in another US patent, US 8227204 B2 "Ionizing-radiation-responsive compositions, methods, and systems" (127).
A synthetic enhancer/promotor containing four CArG elements (E4) functions better than the wild-type human Egr-1 enhancer after a single dose of 2 Gy. It has been used in a radiation-controlled molecular switch for use in gene therapy of cancer (128). It is based on the Cre/loxP recombination system of bacteriophage P1. The radiation responsive promotor controls the expression of the Cre recombinerase which activates a transcriptionally silenced sensitizing gene by loxP site mediated recombination. The CMV IE promotor-enhancer causes efficient sustained expression of downstream genes, the expression is both prolonged and at an increased level. The recombinerase identifies loxP recognition/cleavage sites flanking the stop cassette. The amplification brought about by the molecular switch was about 40-fold compared to non-irradiated controls. The experiment involved transfection with two plasmids.
With "signalling pathways" or "signalling scheme" is defined a schematic description of how and by what means the focused ionizing radiation is translated to necessary biological actions such as entry of the conjugate into the relevant cells and into the nuclei, the attachment of the promotor to its intended site on the DNA, the beginning and the end of the transcription and the detachment of the promotor from the DNA without going into any detail of biophysics and biochemistry.
A prolonged and uninterrupted treatment of deficit volume will in course of time result in conversion of deficit volume to redundant volume and vice versa, a prolonged and uninterrupted treatment of a redundant volume will in course of time result in a deficit volume, lack of temporal category persistence, necessitating the initiation of the antimotif. There is no way to imagine an auto feedback system for the regulation of the OFF-signals, they have to be set "manually" after radiological assessment of the anatomy at the time and the OFF-signals all have to be given at the same time in the form of a global OFF-signal, the administration of detaching molecules.
There is the problem of accuracy, a problem which the natural morphogenesis does not have. Suppose the surface of the proximal femur at the beginning of the treatment is partitioned into areas intended to have osteoblastic predominance, osteoclastic predominance or no dominance of any sort (deficit volume, redundant volume, intermediate volume) respectively where this partitioning is considered to be on the route to the normal anatomy. Will a normal anatomy be the result? No, it will not. The more severe the deformation is the more unlikely it is that a single administration of conjugates will be enough. There will be a need for repeated evaluations with new mappings into areas where an osteoblastic/osteoclastic predominance is needed followed by new administrations of conjugates and radiative ON-signals. NEE has to be performed in steps which is an immediate consequence of the lack of an effective auto-feedback system in the substitute for the natural morphogenesis.
An advantage with the dividing of the treatment into steps is that it is easier to achieve a small change of the anatomy into the right direction, the sum of small steps will eventually establish the normal anatomy, at least in theory. It is presumably easier to keep a functioning promotor in place for a shorter time than for a longer time. A disadvantage is that the total dose of ionizing radiation will be higher.
The dividing of NEE into steps highlights the concept of gene therapy with postmitotic persistence (gene therapy where the effects of the gene therapy is inherited by the two daughter cells when the primary cell, originally subjected to the gene therapy, divides). If the planned duration of the step is considerably longer that the lifetime of the cells (before they divide or die without having divided) it is important that the biological change in the cell brought about by the gene therapy is inherited by the daughter cells, if the primary cells divide, otherwise the effect of the gene therapy will rapidly fade away.
By dividing the treatment into steps where the gene therapy is repeated at the beginning of each step the demand for gene therapy with postmitotic persistence, transductional targeting, might be reduced but it may still be there, that depends on the relation between the duration of a step and the duration of the lifetime of the cells subjected to the gene therapy.
The promotor, in the case of transcriptional targeting, residing in the nucleus must possess a chemical detachability making the promotor detach from the genome and leave the nucleus and the cell when a "detaching molecule", whether it is an enzyme or not, is administrated intravenously/intraarticularly. It is this "detaching molecule" which is used at the end of each step of the treatment as a global OFF-signal to remove all the administered promotors from the hip joint and it is also used to remove all attached promotors in the body if accidentally conjugates should have entered unintended cells.
A naturally occurring mechanism of the cell should not be able to modify, silence or remove an attached conjugate/promotor, only "the detaching molecule" should have that capability. The time to give the global OFF-signal at the end of a step is decided by the anatomy at the time/the algorithm, not by a naturally occurring cellular mechanism. Obviously, the conjugate and the detaching molecule should be non-toxic and non-immunogenic.
The situation could get more complicated if not only the entry-mechanism of the conjugate is switchable but also the promotor is switchable (by radiative OFF- and ON-signals). If that would be the case the promotor could be switched off and on several times during a step. The step could be divided into substeps. A complication is that the OFF-signal must be radiative and not through a detaching molecule because it must be targeting the specific CFU. It is, however, important to keep in mind that the hip joint is not a computer processor which can be programmed at will.
If for instance an initial start signal for motif number 3 has been given to a portion of the proximal femur and at a later evaluation this particular area must be deprived of the effects of this signal but the other areas should be left unaltered it will be given a "temporary-stop" - signal. If at a later evaluation it is considered that this particular area of the surface should resume its motif 3 behaviour it will be given a "temporary start" - signal. At later evaluations there could be further switches between "temporary start" - signals and "temporary stop" - signals, with targeted ionizing radiation (with the consequence that regular check-ups presumably should avoid CT-scans) if that is necessary because of the anatomy at that particular time. It would require knowledge about the precise whereabouts of the different types of conjugates, a knowledge which would have been made possible by an imaging ability to detect the conjugates. A step without substeps has only an element of targeting in the radiative ON-signals, there is no targeting in space in the global OFF-signal in the form of the administration of detaching molecules.
The temporary stop signal and the temporary start signal is given when time has elapsed from the initial start signal at the beginning of a step when there no longer are any conjugates in the systemic circulation. From that point of view it should not be necessary to have a 2-channel system of beams as there are no conjugates in the systemic circulation to consider but a straight line of a beam would most probably, because of the anatomy of the hip joint, before and after it has hit the intended CFU, also hit another part of the hip joint also containing switchable promotors and this would favour the use of a 2-channel system.
With a 2-channel system the initial start signal requires 2 scintillator-photoswitch pairs, the temporary stop-signal requires 2 pairs and the temporary start signal requires 2 pairs, in total 6 pairs.
The photoswitch in the temporary OFF-signal and in the temporary ON-signal directed at the promotor already in place in the nucleus, differs with respect to the duration of the switched state from the photoswitch of the initial ON-signal which permits the entry of the conjugate into the cell. The switching of the photoswitch of the two temporary signals must be permanent or at least have a duration up to the opposite signal is given if the same photoswitch is used for the two temporary signals, P-type photochromism. The temporary OFF-signal must cause an OFF-state of the promotor until the temporary ON-signal is given and vice versa. Therefore azobenzene, with a half-life of its cis-state of ms-days depending on its chemical environment, T-type photochromism, cannot be used.
With the availability of temporary OFF-signals and temporary ON-signals, each radiative in nature, each step is divided into substeps which would give more flexibility to a step in the sense that a motif in progress could be temporarily halted. Further flexibility with the access to the antimotif would require another kind of conjugate/promotor.
Without the availability of substeps a global OFF-signal is given to end a step when somewhere in the joint lack of temporal category persistence (TCP) is imminent. The area of the hip joint where lack of TCP is not imminent also will be deprived of its promotors only to receive the same type of radiative ON-signal and promotor as before. This process is repeated so the number of steps could be almost infinite.
The availability to make a temporary halt at a particular CFU would make the step monotonous while in the absence of temporary stop and start signals the step would be strictly monotonous (the terminology is from the description of functions in mathematics). A monotonous step gives more flexibility to the treatment but is technically more demanding than a strictly monotonous step.
A unidirectional strictly monotonous step is a step which can accomplish a motif but not its antimotif and which has not the availability of temporary OFF- and ON-signals, i.e. it has not the potential of using substeps.
A unidirectional monotonous step is a step which can accomplish a motif but not its antimotif but has the availability of temporary OFF- and ON-signals, i.e. it has the potential of using substeps.
A bidirectional two-sided monotonous step is a step which can accomplish both a motif and its antimotif where both the motif and the antimotif has access to temporary OFF- and ON-signals, i.e. the potential of using substeps.
A bidirectional one-sided monotonous step is a step which can accomplish both a motif and its antimotif where only the motif or the antimotif (but not both) has access to temporary OFF- and ON-signals, i.e. the potential of using substeps. It is equivalent to a bidirectional one-sided strictly monotonous step.
A bidirectional two-sided strictly monotonous step is a step which can accomplish both a motif and its antimotif where neither the motif nor the antimotif has access to temporary OFF- and ON-signals, i.e. the step has not the potential of using substeps, except from the direct switching to the antimotif.
The use of substeps, i.e. the use of temporary OFF-signals and temporary ON-signals, could make "the signalling scheme" and the resulting structure of the conjugate quite complicated. It could become a puzzle and the reason for that is that NEE is a second-generation principle. A third-generation principle of eliminating the deformation of the hip joint after LCPD uses the guiding mechanisms of morphogenesis where everything takes care by itself but a theory for a third-generation principle does not exist. NEE substitutes the guiding mechanisms of morphogenesis with focused beams of ionizing radiation, at least in theory, to have it performed in reality is quite another matter.
There are not only one but there are two articular surfaces the anatomies of which are to be corrected. These two articular surfaces are in direct contact with each other and the joint is loaded by the body weight.
In the first generation of principle for correction of the deformation of the hip joint after LCPD a reference form is used. This reference form obviously is necessary to secure the normal anatomy of the hip joint.
The closest to a reference form the second generation of principle has to offer is the opposite articular surface. The question is what importance the opposite articular surface might have on the other one to attain the normal anatomy considering that a small change in the anatomy of one articular surface will be sensed by the opposite articular surface (mechanotransduction) and eventually lead to adaptive changes and must be taken into account when planning the path to the normal anatomy.
The type of influence on the anatomy of the opposite articular surface the articular surface might have in the long run is to reduce the redundant volume and possibly to increase the deficit volume. If for instance a motif 1 was in progress in the femoral head it could in course of time be sensed in the acetabulum as a pressure and lead to adaptive changes as a response to the localized increase in volume of the femoral head. One could compare with the lateral flattening of the acetabulum as a result of the compression and the flattening of the femoral head visible on the anterior-posterior X-ray caused by LCPD. It will not be a diminishing of the deficit volume of the opposite articular surface, the influence/interaction is through pressure, not traction. If that should be the case that there is such a contribution as regards the influence on the anatomy, except for the motifs in progress, it should be incorporated in a "control system", an algorithm. (Control systems are mathematical procedures, algorithms, used in industry to control processes). Conditions imposed upon this algorithm ("from point to three-dimensional surface in incremental mode") is that in the end the articular cartilage should cover the two opposite articular surfaces, weight bearing should be allowed during the treatment (to walk on crutches for 5-10 years is unrealistic or at least a serious drawback) and that the successive changes in anatomy should not make the adaption of the vascularization more difficult. The algorithm when applied to each of the steps of the treatment will more or less automatically lead to the normal anatomy of the hip joint. In this case it would be a complicated situation involving two three-dimensional surfaces interacting with each other and under the influence of motifs in progress where the goal is to achieve the normal anatomy of the hip joint.
The elimination of redundant volume through pressure from the opposite articular surface caused by an advancing motif could equally well be accomplished by a retreating motif (elimination of redundant volume) but the question is if pressure from the opposite articular surface will facilitate a retreating motif, if it will make it progress faster. If that should be the case it should be taken into consideration by the algorithm.
If the deformed anatomy of the proximal part of the femur is denoted by "surface F", its normal anatomy is denoted by "surface FN", the deformed anatomy of the acetabulum by "surface A" and its normal anatomy is denoted by "surface AN" the task is to convert surface F to surface FN and surface A to surface AN. To define the goal of NEE is a piece of cake. These two conversions will not be performed during one step but in a necessary number of steps.
If "n" is the number of steps the anatomy of the proximal portion of the femur will have to go through we get the sequence F = F0 , F1, F2 , , , Fn-1 , Fn = FN, and with the same number of steps the anatomy of the acetabulum will go through A = A0 , A1 , A2 , , , A n-1 , An = AN where the subscript 0 denotes the start anatomy, i.e. the original deformed anatomy. The subscripts 0, 1, 2, ... , n-1, n denote the number of steps which have been performed.
The gradual reduction of the deformation of the hip joint can also be described by the sequence
D0, D1, D2, ... , Dn-1, Dn = 0 where Di is the deformation (the sum of the absolute value of the deficit volume and the absolute value of the redundant volume of the hip joint, including both the proximal portion of the femur and the acetabulum) where the subscript denotes the number of steps which have been performed at the time of calculation, Di < D i-1.
Osteoblastic/osteoclastic predominance will constitute "a leading force" and moulding will constitute "an adaptive force" in the normalization of the hip joint anatomy.
NEE, a hypothetical treatment, is associated with several difficult/impossible problems. Some of them have already been mentioned during section 2, outline of NEE, and they will be repeated here in a little bit extended version.
NEE is the combination of a targeting system with two sets of beams and conjugates and its application area, gene therapy in bone and articular cartilage. This combination presents five obstacles. The first is that such a targeting system does not exist. Scintillators are used on a macro-scale, for example in high energy physics to detect particles/radiation but for NEE they would be used on a molecular scale which would make the absorption too low. It would require a very special scintillator yet to be invented. Radiotherapy uses targeted ionizing radiation but there are no scintillators or photoswitches involved. The targeting in space is not with reference to the whole of an organ such as the liver, kidneys or lungs (in the case it should exist a cell membrane receptor only found in that particular organ) but the targeting in space is related to a specific part of the organ (the skeleton) obtained by the subtraction of two volumes. The demand that the targeting system (beams, scintillators and photoswitches) should be a "2-channel system" with the effect that the targeting is "pointwise", i.e. the activated conjugates occur only at the focus of the beams and not along the entire path of the participating beams is yet another problem.
The second obstacle is associated with the application area, articular cartilage does not have blood vessels and the intercellular substance is penetrable only for small molecules, gene therapy cannot be effectively performed in articular cartilage, particularly not in vivo. Knowledge about bone and cartilage will increase and gene therapy, photochemistry, scintillators, optogenetics and nanotechnology will continue to develop in the future but something which will not change in the future is the fact that articular cartilage has no vessels and that the hydrodynamic radius of the intercellular substance of articular cartilage is about 4-5 nm. Associated with this biological obstacle is the question of stem cells, growth velocity and growth factors. Dedifferentiation of adult articular cartilage (the readiness to initiate growth in the adult, not the conversion of chondrocytes to fibroblasts in a cell culture) and the spatially controlled initiation of growth through superficially located stem cells in the articular cartilage is on the menu of impossibilities. There must be a presence of stem cells in the superficial part of the articular cartilage which can initiate growth to eliminate deficit volume. Even if there would be any stem cells left, a hypothetical assumption, there is the question of growth velocity, i.e. if the growth that can be initiated is high enough and can be sustained long enough to be of any use. The growth factors/promotors also must be defined.
The third obstacle, related to the above, is associated with the proposed principle itself, i.e. to substitute morphogenesis with remote control of gene therapy in bone and articular cartilage where the remote control is achieved by two sets of beams with X-rays or gamma-rays and conjugates in a stepwise fashion is a crude and most probably an insufficient method. The remote control would operate in a discrete mode but morphogenesis operates in a continuous manner and has an inbuilt feedback system. The step by step remote control of the gene therapy could have its discrete mode of operation changed to a continuous mode of operation by making the steps smaller in time to finally be infinitely short but that would make the dose of ionizing radiation infinitely high. To try to create a substitute for the natural morphogenesis which will function in the adult patient is to have high ambitions.
A fourth obstacle is to keep the treatment targeted, i.e. there should not be any activated conjugates outside the intended CFUs, especially not disseminated throughout the whole body.
A fifth obstacle is the fact that a serious side effect of ionizing radiation is that it can cause cancer. The fourth and fifth obstacles are related to safety or risks of the treatment.
We have come to the end of the road with the realization that NEE is impossible, a realization we already had at the start of our creative and ground-breaking work. We have constructed a theory, incomplete and insufficient, for the elimination of the deformation of the hip joint after LCPD. The theory necessitates specific capabilities which do not exist. Nanotechnology for medical applications ("nanomedicine") to some extent deals with cellular and organ-specific targeting of drugs (129). In that reference there is a chapter on targeting of the brain using a magnetic field and elsewhere in the text there is mentioning of electric field and ultrasonic field as methods of targeting. There is not, however, mentioned anything about focused beams of ionizing radiation as a means of targeting. There are limitations to what sensible people suggest in a scientific context. Another capability desired also by others is gene therapy in articular cartilage. If gene therapy in articular cartilage was possible and believed to be of any use in the treatment of arthrosis the interest would be immediate and global, for other genetic diseases in articular cartilage too. We have arrived at obstacles which also others are struggling with. We have devised a theory necessitating capabilities which others would find interesting. A research problem in a medical application may be of the same nature as a research problem in another medical application. Everything is interconnected.
NEE offers many opportunities to a nice chat about bone and cartilage biology, synchrotrons, Monte Carlo transport of photons and electrons, atom physics, molecular physics, wave-matter interaction, radiobiology, scintillators, photoswitches, stem cells, senescence of chondrocytes and in vivo gene therapy in bone and cartilage tissue engineering at the afternoon tea. An assiduous study of these subjects will make the student knowledgeable and prevents many occasions to blameworthy and sinful behaviour as well as any other spare time for the next hundred years, just in time to answer the question "what have we learned?" at the next centenary (130). A subscription to these centenaries could be placed in the bookshelf for future study. X-rays were discovered in 1895, the search for scintillators began immediately and in 1896 CaWO4 was used to detect X-rays. LCPD was first described in the beginning of the twentieth century. Synchrotron radiation was first detected in 1947. The determination of the chemical structure of DNA took place in 1953 after which molecular biology was born, gene therapy arrived later. Fritzsche in 1867 demonstrated for the first time a reversible photoinduced transformation between two metastable states of a molecule, tetracene, optogenetics has evolved after the year 2000. In this context these time periods are short but after a millennium the complete set of centenaries will represent a vast amount of knowledge in science and may be used to make an update on the possibilities of NEE.
The intricacies will be sorted out by the orthopaedic surgeon who resolutely shovels the prosthetic joints aside and majestically enters the arena where he will enlighten us, guide us in our pursuit of knowledge, save us from our pitiful ignorance, impress and bless us with his knowledge in relevant sciences, let his mere presence raise us to a higher state of sublimity, climb down from Heaven like an Aristoteles to a chorus of angels and present us with the Revelation and, as a bonus, on the closing day enter the city on a white horse to receive the jubilations of the people and cover himself with glory and because these subjects are well accommodated in the curriculum of the medical faculty and are well-known to every medical student that should not be a problem. To the tunes of the London Philharmonic Orchestra coffee and sandwiches are served during the pause along with a free ticket to the celebrations in Athens, hotel, three meals a day and sightseeing included.
Stalin's speech in Athens. The hydrogen in the sun will last for another billion years. When that time comes it would be appropriate to celebrate the event at the Dionysus theatre in Athens where the Greek tragedies were presented during classical antiquity. The spectators will be thrilled by the expected gala performance on the history of mankind and to hear about the new wonderful planet they were going to inhabit. How disappointed they will be when instead of the actors Josef Stalin, temporarily resurrected for the benefit of the celebrations and with a leash in his left hand tied to a New Zealand white rabbit chewing on a carrot and worriedly looking at the distant red disk which lately has been enlarging, enters the scene and says: "I haven't understood why you are hanging about here. You are obsessed. You are obsessed with the loading of all sorts of metallic and plastic materials into the human body regardless of if it is arthrosis or the cat has run away. These devices might well be suited to repair my car but not your persistent and well documented inability to adopt a biological approach. There are no vessels in articular cartilage, the hydrodynamic radius is only about 4-5 nm and there hasn't been published a single book about articular cartilage containing a chapter on in vivo gene therapy of both articular cartilages in a joint so I can't see that there are any reasons for You to continue the story." It has not yet been decided whether Rembrandt or Francisco de Goya will be assigned the task to paint this scene.
"The mind struggles to establish a connection-a sequence of cause and effect-and, being unable to do so, suffers a species of temporary paralysis."
The Gold-Bug
Edgar Allan Poe
It is understandable to find the idea of an "ACPS-measurement" as a prerequisite for finding the cause of the disease, and NEE at the same time. When reviewing the literature on the cause of the disease you will sooner or later give up and revert to "basic principles", i.e. you must know what comes first, the ischemia or the fracture. You turn it around, i.e. you do not try any longer to find the cause of the disease with the unspoken assumption that it is possible to find the cause of the disease. Instead you switch this unspoken assumption to the assumption that it is impossible to find the cause of the disease and you motivate it by the fact that it is impossible to perform an ACPS-measurement. You close the case as regards finding the cause of the disease, you do not want to have anything to do with it any longer because you believe that any attempt to find the cause of the disease will fail. It will fail because it is impossible to perform an ACPS-measurement. The hundred years which have passed since the first description of the disease do not contradict the assumption that it is impossible to find the cause of the disease. In quantum mechanics an observation can interfere with a system which gives rise to the uncertainty principle, exact and simultaneous knowledge about two quantities such as position and momentum of a particle may be impossible. As regards the aetiology of LCPD the necessary observation itself, the ACPS-measurement, is impossible. However dear it would be for you to be able to perform an ACPS-measurement you have to come to terms with the fact that it will never be possible, however sad that might be for you, there is nothing you can do about it. If the assumption that it is impossible to find the cause of the disease because it is impossible to perform an ACPS-measurement is accepted the attention will be shifted from the cause of the disease to the deformation itself and this deformation will be considered to be inevitable and has to be dealt with in its own right. This view on LCPD is hidden and it must be extracted. It is a way of looking at things. Why bother to try to find the cause of LCPD when it is impossible because it is impossible to perform an ACPS-measurement? Experiments and measurements constitute the foundation of the scientific method. You cannot establish the cause of LCPD because it is impossible to perform an ACPS-measurement, it is as simple as that. orthopaedic surgeons have for more than a century been staring at the X-rays of hip joints afflicted with Perthes disease and these X-rays have been staring back at the observers and an answer has never been found. It is an absurd situation and it will continue to be an absurd situation because an ACPS-measurement will never be possible. As for the aetiology of the disease, relax, buy a house at the coast in Spain and watch the sea instead. Mm?
During the 1930's there was a young and promising doctor who had completed his training as a radiologist at the age of thirty. He was bright so he understood the meaning of the words "cause" and "effect". The staff of the department were proud of having such a bright doctor among them and they were convinced he was going to perform great deeds. He took an antero-posterior X-ray and a Lauenstein projection of the affected hip-joint of a patient with LCPD. He observed that the femoral head was flattened, i.e. there had been a fracture, or several fractures, of the femoral head. He also observed that there was an increased density of the bone tissue of the femoral head, and fragmentation, as a sign of ischemia and resorption. Then he took a sheet of paper and drew a horizontal straight line symbolizing an x-axis, in this case a time-axis, as he had learned in school. He made a little vertical mark on the x-axis and wrote the word "fracture". He drew a little vertical mark to the left of the first one and wrote the word "ischemia" and thought: "Perhaps the ischemia comes first and the fracture is a result of the ischemia." He thought about this for a while and then he looked unsure of himself. He drew a little vertical mark to the right of the first one on the x-axis and again wrote the word "ischemia" and thought: "Perhaps instead the fracture is the cause and the ischemia the effect". He did not know which of these two alternatives was correct and decided to solve this mystery by an intense study of these two X-rays. He was a man who did not stop short of attending to difficult problems and he set to work with determination and diligence. The staff took off their shoes and tip-toed when walking past his office in order not to disturb him in his intense studies of these two X-rays. He devoted himself to this problem for the rest of his occupational life which lasted until he was eighty years old. He came to work at eight o'clock in the morning and left work at 17 o'clock in the afternoon and he studied these two X-rays every working day during these fifty years. He did not manage to solve the problem.
To summarize, the overall goal in the management of LCPD is the absence of deformation of the hip joint. In an effort to achieve this goal the first principle is to treat the disease in order to avoid any deformation which often is impossible. The second principle would be to look at the cause of the disease but as it is impossible to perform an ACPS-measurement that is impossible. There is no mutated gene (or a set of genes) which has a hundred percent specificity or sensitivity for the disease. The third principle is to treat the deformation itself in order to eliminate it. These three principles together constitute "the trinity of LCPD". When looking at how such a treatment of the deformity would be performed there is a classification of principles into three generations. The first generation of principle would be surgery. The second generation of principle, NEE, rests on the fact that the hip joint exists, i.e. it has been created by the osteoplastic envelope, periosteum, epiphyseal cartilage and articular cartilage and the bone cells and chondrocytes do not lose their nuclei during maturation as is the case for erythrocytes and keratinocytes. The osteoplastic envelope is the object of NEE. NEE is the subject of this article to be handed over to a young and promising orthopaedic surgeon prohibited from leaving the premises before the fulfilment of the commission in obedience to Stalin. After the fulfilment of the commission he should be met with tolerance and understanding and be given proper rehabilitating treatment at a rest home at the sea at the expense of the state. The third generation of principle to eliminate the deformation, also using the osteoplastic envelope but with an intrinsic and not an extrinsic guiding system, rests on the fact that the information directing morphogenesis resides in the genes and the genome is still there but a theory for this cannot be constructed. To imagine that the physician would make a magic gesture over the hip and to pronounce a secret incantation to oblige higher powers of morphogenesis with the result that after five years the deformation would have vanished does not qualify as a theory, it has to be more specific.
As the first stage in NEE there is the analysis of the deformation and its classification as deficit and redundant. There is the identification and classification of the processes which are to take place, the four different motifs. The substitute for the guiding mechanisms of morphogenesis encompasses two sets of beams of ionizing radiation giving start signals, a conjugate with two scintillators, two photoswitches, a switchable cell-entry function and a chemically detachable promotor. The treatment is divided into steps guided by a controlling algorithm, each step beginning with the administration of conjugates, followed by radiative initial ON-signals and ended by the removal of the conjugates by the administration of a detaching molecule, a global OFF-signal. The CFUs, the points of focus of the beams, are classified into direct points, indirect points and boundary points and internal points. NEE is a combination of a targeting system and the application of this targeting system to gene therapy in periosteum, bone and articular cartilage. A menu of impossibilities, obligatory when discussing NEE, has been set up and has confirmed the conclusion that NEE is impossible. NEE bypasses the aetiology but is impossible. An elementary history of relevant sciences with some dates for important scientific milestones has been provided as well as an estimate for the suitable time lapse to the next evaluation of the possibilities of NEE, which because of the special character of the problem has been set to a thousand years. This is a long time to wait and to entertain us the subscription to the centenaries will have exclusive rights to the future adventures of our fairy tale orthopaedic surgeon and his life companion, soon to be described, as well as the future of another even more complicated project currently in progress so we may look forward to a long-lasting amusement.
If the alternatives treatment of the disease, aetiology of the disease including genes and NEE ever will achieve the overall goal, the normal anatomy of the hip joint throughout life, and if that should be the case, which alternative has the best possibility to achieve this goal is a question which will not be answered in the foreseeable future. The question can be rephrased to which of the three alternatives surgery, NEE and morphogenesis has the best prospects in the long-term future of eliminating the deformation of the hip joint caused by LCPD.
Anyone who has the intention to set up a department of optogenetic orthopaedics might encounter introductory problems. If these problems are greater than the problems anyone would have who had the intention to explain how the putting forward of a mutated gene as a cause of LCPD possibly could achieve the overall goal, the normal anatomy of the hip joint throughout life, remains to be seen. The comparison is also applicable to the treatment of the disease including patients who present a deformation of the hip joint already present at the time of diagnosis. Classical orthopaedics is inadequate in this context. Having the three alternatives treatment of the disease, the aetiology of the disease including genes and NEE on the table the question can always be put, the comparison can always be made.
Geometric reversal. The classification of generations of how to eliminate the deformation of the hip joint after LCPD: surgery, NEE and morphogenesis, will be updated if "geometric reversal" is included. Then "geometric reversal" will be the third generation and morphogenesis will be the fourth generation.
For a more pronounced deformation the femoral neck angle is decreased. The normal sphericity of the femoral head is lost and replaced by a flattening of the femoral head. The normal spherical concavity of the acetabulum is lost as an adaptive consequence of the flattening of the femoral head and replaced by a flattening of the acetabulum especially in its lateral part. Geometric reversal, which does not use ionizing radiation, addresses each of these three parts of the deformation by a "procedure". These three procedures are appropriately coordinated with each other in time.
The first procedure is the correction of the femoral neck angle, use the fovea capitis as a guide point.
The second procedure is to create a spherical femoral head. The primary part of this procedure is to perform a local injection of a collection of appropriately gene-manipulated bone cells capable of proliferation, in the centre of the future localization of the femoral head. These cells will have the capacity to proliferate in a spherical manner, to replace neighbouring bone tissue without causing an increased risk of a fracture of the femoral head, to incorporate existing vascularization and to attach to the articular cartilage when it reaches it, the articular cartilage itself will adapt to the spherical shape and the growth is stopped by an intravenously administrated signalling molecule when the femoral head has attained its normal anatomy. One can compare with an osteoma, radiographs of osteomas, however, show that osteomas do not have exactly spherical contours. If the centre of the future femoral head is located outside the boundaries of the deformed femoral head the procedure has to be repeated. The secondary part of this procedure is to remove the redundant volume.
The third procedure is to reestablish the spherical concave surface of the acetabulum. Weight-bearing and movement in the hip joint will through pressure-sensors aid in the normalization of the spherical form when the femoral head gets rounder.
To make this application of "synthetic morphogenesis" (131) or "orthopaedic synthetic morphogenesis" (OSM) /tissue engineering a clinical reality is left to the reader as an exercise.
3D-printing in the industry began in the 1980s, "additive manufacturing". Around 2009 consumer 3D printers arrived at the market. There are two kinds of them, FDM printers (fused deposition modelling) and SLA printers which use resin for stereolithography (SLA).
An FDM-printer uses an extruder which grabs the filament (materials of various kinds to be printed) from a spool, heats it and passes it through a narrow nozzle to the building plate. Stepper motors vary the position of the extruder (or the building plate) in x-, y- and z-positions. A fan controls the cooling temperature of the newly deposited material.
A SLA-printer uses a liquid resin (polymer) instead of a filament from a spool. The liquid resin hardens ("cures") layer by layer when ultraviolet light is directed to it.
What is to be printed is a 3D-model, usually in STL file format, STL = STereoLithography or Standard Tesselation Language which defines points in space. These points are connected to triangles. In this way a "mesh" is formed which defines the outward border of the object. The 3D-model is created in a CAD-program (Tinkercad, Meshmaker, Fusion 360) and saved as an STL-file. The STL file is then sent to a "slicer"-program which cuts the 3D-object into "slices", in g-code, which are used by the 3D-printer to lay down one layer after the other (132).
As regards 3D-printing in medicine with the exception of bioprinting (133) the most common technologies comprise vat photopolymerization (a light source causes a chemical reaction in the resin causing it to become solid), material jetting (the jetting of microdroplets of liquid photopolymer resin onto a build tray), binder jetting (the jetting of a liquid binding agent on to a bed of a fine powder in the shape of the currently printed layer of the object), material extrusion (the same principle as for FDM-printers in the consumer market) and powder bed fusion (a high-power laser or electron beam fuses small particles of plastic, metal, ceramic or glass).
Planning before resection of bone lesions, repair and replacements of joints, correction of congenital deformities and surgical management of osseous trauma are fields of application for 3D-printing in medicine. CT and MR images can be used for printing of orthopaedic models. 3D-printing can also be used for educational purposes with reference to human anatomy. Concrete clinical examples of 3D-printing are facial augmentation with silicone implant, hemi-pelvis reconstruction with 3D-printed titanium implant, revision hip arthroplasty, directly 3D-printed cranioplasty in PEKK (polyether ketone ketone), temporomandibular joint and mandibular reconstruction, machined PEEK zygoma implants, directly 3D- printed titanium mandibular reconstruction plate, patient-matched orbital floor implant, salvage ankle fusion cage directly 3D-printed in titanium, distal humeral resurfacing implant directly 3D-printed in titanium and 3D-printed, bioresorbable tracheal splint for tracheobronchomalacia.
AM (additive manufacturing) and TE (tissue engineering) have been combined to create 3D-bioprinting (134). The main categories of 3D-printing are extrusion-based methods, droplet-based methods and energy-based methods (application of light or heat).
"Embedded bioprinting" allows for printing of vessels. A support material surrounding a branching and rejoining void space in printed in which a "sacrificial" or "fugitive" bioink is printed. The fugitive material is later removed. A coaxial, or concentric, nozzle may be used for this purpose. The fugitive bioink is printed through the inner lumen of the nozzle and the supportive bioink is printed through the outer lumen, the lumen between the two short tubes of the nozzle. Bioinks can be scaffold-free consisting of aggregates of cells and scaffold-based which consist of biomaterials with encapsulated cells. Cardiac patches and a small heart have been 3D-printed (135) as well as tissue mimicking the function of lungs (136), and articular cartilage (5).
[1] There is also a generation 0 (generation zero) principle and this was conceived by looking at fig. 15-4 on page 382 in Histology (137) showing a long bone which has been decalcified and tied into a knot. The principle would be to establish an extracorporeal circulation for the hip joint with erythrocytes or fluorine-carbon compounds (perfluorocarbons) as oxygen carriers, use EDTA to decalcify the joint, perhaps use ultrasound to increase the solubility of the mineral, hydroxylapatite, to apply a reference form to secure the correct anatomy and then to re-calcify the joint. Organic bone matrix is elastic, not plastic, and the vessels will be compressed during the procedure. This principle will not be mentioned any more.
[2] No callus at fractures of the femoral neck in the elderly, also not in the young patient? Fractures of the femoral neck are uncommon in young patients. Disappearance of the periosteum of the femoral neck during growth, if there ever has been one? The femoral head has been subjected to an ischemia during LCPD so even if there has been a periosteum covering the femoral head outside the articular cartilage and the femoral neck perhaps it has been destroyed during the disease period? Perhaps a contribution to the width of the femoral neck by the epiphyseal growth cartilage?
[3] A scalar (a number, for example 1,2,3 etc.) is a tensor of rank 0, a vector is a tensor of rank 1. An example of a tensor of rank 2 is the stress tensor represented by a 3 x 3 matrix.
[4] The K-shell is the innermost electron shell of the atom. The different electron shells (K, L, M, ...) correspond to the principal quantum number n. The quantum numbers (n, l, m) arise in the solution of the Schrödinger equation (138).
The speculations concerning treatment of the deformation of the hip joint after LCPD are theoretical and do not describe treatments which exist in any medical service system. These treatments, as they have been outlined in this article, do not exist in reality, not in any part of the world.
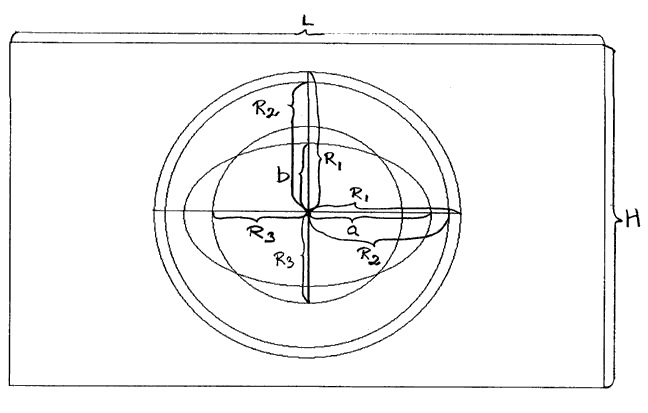
2πR1= L + H 2πR3= L L/H = (L+H)/L a/b = (a+b)/a
(a-R3)/(R2-a) = ((a-R3) + (R2-a))/(a-R3) = (R2-R3)/(a-R3)
(R2-a)/(R1-R2) = ((R2-a) + (R1-R2))/(R2-a) = (R1-a)/R2-a)
The cillipse (circle + ellipse). The femoral head is round, the deformed femoral head can symbolically be represented by a deformed circular disc, an ellipse. Light can be circularly and elliptically polarized.
*** 2014, 2017, 2018, 2019, 2020 ***
Once upon a time there was an orthopaedic surgeon who believed that because he had studied at the medical faculty he had all the knowledge anyone ever could imagine and wish for. His idol was Napoleon Bonaparte and he had a portrait of Napoleon hanging on the wall in his home and even a Napoleon hat and sometimes wore it at work which caused embarrassment of his colleagues and curiosity of his patients. His favourite film was Napoleon by director Abel Gance, it was a silent film but he loved the sceneries and old costumes. Because of his admiration of Napoleon Bonaparte he got the nickname "Napoleon". The only thing he feared was the ward sister who was a huge woman with great bodily strength and a bad temper, no one dared to quarrel with her.
He had the view that all problems could be solved by prosthetic joint replacements. If there was political unrest somewhere the fighting parties should have prosthetic joint replacements. If the weather was bad the weather forecaster should have a prosthetic joint replacement and if the cat had run away the cat should have a prosthetic joint replacement. Sometimes when he during a prosthetic joint operation had removed a piece of bone, for example a femoral head, he got ecstatic, he growled showing his fangs and triumphantly raised it towards the ceiling in honour to Napoleon Bonaparte in a similar way the Aztecs had done several hundred years ago when they had cut out the heart of a captive enemy as a sacrifice to their Sun-God Huitzilopochtli. It was rumoured that he once during an operation had put a femoral head in his mouth, pierced it by his fangs, left the operating theatre, walked to his office to put on his Napoleon hat and then left the hospital to head for the city square. It must have been strenuous for the poor inhabitants to see an unresponsive man dressed for surgery with a Napoleon hat on his head and a femoral head in his mouth walking about in the city square constantly growling. That was not a way how to behave. What would they think of the hospital? After a couple of days in the psychiatric ward his behaviour returned to normal and he could work again.
His favourite author was the science fiction writer Isaac Asimov and he had the dream that the human being could be replaced by a robot. The replacement of a joint with a prosthetic joint was the first step in his grand plan to replace the whole human being with a robot. The traditional approach had been to study diseases with the aim of finding a cure for them but history had shown that this was too time consuming and difficult a process. Napoleon's approach was instead to study the human being and to improve it by transforming it to a robot which was less amenable to disease. The great advantage of this plan was that the pathological panorama could be reduced or even eliminated. If a part of the robot did not function properly it was only to replace it. It then would be easier to be a physician. He was amazed that no one had come up with this idea before. He concluded that his ability to see the obvious was an expression of his genius. There was the problem of cognitive functions and emotions but he assumed that could be managed by a powerful central processor and some artificial intelligence. As for the replicative function of the human being he had heard of self-assembling nanostructures so that function could probably be substituted too and would facilitate life in several ways. When he was submerged in these plans he looked determined and always had his Napoleon hat on and his patients had to watch out so that they did not leave the examination room as robots. When thinking about this project he looked dreamingly at the portrait of Napoleon, swirled his glass of brandy and said: "My indisputable greatness must become known to everybody. We will conquer the world!" The project got a push forward in 2003 when the first airborne division of orthopaedic surgeons with Napoleon hats was dropped in Kent fighting their way to the outskirts of London. Never had there been such ardour in human behaviour since the storming of the Bastille. Their use of arms such as catapults, pea-shooters with homing peas, in this context they had indeed embraced the idea of targeting, and the final pillow fight inspired their opponents with respect. The situation got so tense that the ward sister had to be called in. When she threatened to unleash her great bodily strength they calmed down and returned home.
He could calculate with three-digit numbers, he knew what a lever was and he had invented his own nail, the latter with a spin-off in the form of impeccable repairs of the fence and roof of his cottage. Because of these achievements he was awarded a ten-year subscription to Donald Duck by the King, a gift that he appreciated. His greatest pleasure during weekends was to read these comics. His teachers in school had told him it was important to read in order to widen his intellectual horizon and there were many funny pictures to look at. He also was appointed cardinal in orthopaedic surgery by the Pope so now he had both a Napoleon hat and a cardinal hat. The appointment took place in St Peter's Basilica in Rome. It was a memorable event not least because of the presence of the Kaiser of Orthopaedia, great-grandson of Kaiser Franz Josef of Habsburg, and his entourage including his dog which was barking at everyone. With pomp and splendour, the Kaiser arrived at the Basilica in his wagon drawn by six white horses, and he was greeted by a cheering crowd and an orchestra playing the Königgrätzer Marsch. He was dressed in an awe-inspiring uniform with countless medals on his chest, one for every nail he had invented, magnificent plumes on his head and a parrot on his shoulder reciting directions for use for the nails. The Kaiser later replaced Königgrätzer Marsch with a more appropriate piece of music when he learned the history behind it. In possession of such prestigious hats as the Napoleon hat and the cardinal hat Napoleon was bound to be met with admiration and respect wherever he went as long as he did not try to put the two hats on his head at the same time. At home he often wore his cardinal hat and admired himself in front of the mirror from different angles. The stance of the church as laid down during the Vatican Council in 1927 and expressed in the orthopaedic confession of faith was that forgiveness of sins and eternal life for an orthopaedic surgeon was achieved by his unquestioning and obedient loading of the quotas of metallic and plastic materials into the population prescribed by the secular government and supplied by the Vatican Mining and Production Ltd. An improved annual report of the company was always welcomed and generously rewarded.
Encouraged by his enhanced status as a cardinal he applied to the Pope for a summer school at the Istituto di Matematica Avanzata where they taught how to calculate with four-digit numbers. His application was treated favourably. The summer school lasted for six weeks and during the weekends he and his fellow students visited an amusement park to buy balloons and to have cotton candy, and to sit on a horse on the merry-go-round and to go for a ride in the roller-coaster was exciting and the highlight of the day. One weekend when he already had had all these amusements he sat down in a sandpit and played with his carpenter toy set he had brought. The passers-by smiled at him. He demonstrated such a virtuosity in the handling of these tools that they understood he had spent much time to become so skilled. The toy set had been given to him by his parents as a Christmas present.
When he became a teenager, he did not want to go out with girls or steal apples from a garden somewhere, no, he only wanted to sit in a sandpit and play with his carpenter toy set as he always had done. He believed that this was what life was all about and he was not able to think about anything else. Sometimes his mother would worry about him. "Why don't you go out with girls or steal apples from a garden somewhere like all the other boys?" she would say. "I like it better here where I can play with my carpenter toy set" he would answer. Because she was an understanding mother she let him just sit in the sandpit and be happy.
Among the passers-by there was a painter who made a painting of this scene. In the foreground Napoleon sitting in a sandpit playing with his carpenter toy set and in the background a merry-go-round where a little boy is busy calculating the centripetal acceleration and a girl sitting in a wagon of the roller-coaster happily waving at the observer of the painting while her friend calculates the relativistic length contraction caused by the high speed of the roller-coaster, it was quite funny actually. The painting was first to be seen in the National Gallery but due to public criticism later sold to a private collector, not everybody thought the painting was funny. During the course the students were given a state of the art minicalculator using the four rules of arithmetic and up to four-digit numbers and he could manage his minicalculator all by himself.
After the successful completion of the course he was happy as a child and he knew his mother was going to be mighty proud of him. It was a great day for a great man. There had not been seen such greatness since the days of Napoleon Bonaparte. He thought it had been a good investment to have attended this summer course in mathematics so that he could read and understand texts in science which would benefit him later in life. Now when he could calculate with four-digit numbers he was certain that he could master any branch of science necessary to transform the human being to a robot. The world lay at his feet. He was going to be victorious. When he returned to work the nurses thought he was a real cutie when he proudly demonstrated how to calculate with four-digit numbers. They celebrated the event with fruit drink and buns. He thanked them by giving a two-hour lecture on the topic "My Greatness" and they realized that he was a profound man. The next day at the morning conference he turned up in a Roman emperor costume which was pointed out to him by one of his colleagues along with the fact that his presence was better appreciated when he was sober. When he realized his mistake he quickly returned to his office and changed to a complete Napoleon outfit including his Napoleon hat. He walked back to the conference room, he stood up on the conference table and he demanded that his colleagues should acknowledge his greatness.
He was an excellent diver. He had the gold medal from the world championships in orthopaedic diving 2005 in Barcelona. From the 5-metre platform he did a backward 2 1/2 somersault with a twist and while passing the 3-metre springboard he performed a prosthetic joint replacement on a patient lying on it. It was the fastest prosthetic joint replacement ever performed and he had a clean entry into the water without a splash. He received the highest score from all the seven judges.
He was very content with himself. After all, he had studied at the medical faculty, he had both a Napoleon hat and a cardinal hat and he had a gold medal from the world championships in orthopaedic diving. What more could there possibly be to achieve? Well, of course, there was the transformation of the human being to a robot and he looked forward to that.
In the evening he was tired and he went to bed. He brought forward his prosthetic joint, kissed it and hugged it. He had been introduced to it at a party by another orthopaedic surgeon who thought he ought to have a life companion. They immediately fell in love with each other and since then they had been inseparable. Everybody thought the two lovebirds were such a beautiful couple when they went for a stroll in town. Had the romantic poets Byron, Shelley and Keats witnessed this they would have been delighted. In the care and affection of his beloved he fell asleep and he dreamed sweet dreams about the promised land where all the human beings had been transformed to robots and he and his life companion lived happily together ever after.
The nail Napoleon had invented and which had aroused such an interest in the Vatican and had made him a cardinal was considered to be a major breakthrough in orthopaedic surgery. It could both take off and land vertically and it was possible to tune in any radio station so the patient could listen to his favourite music at any time. He was invited to a nearby hospital to give a lecture on his nail. The event turned into something like a religious revival meeting. At the end of it he got a burst of applause during ten minutes and they all looked as if they had seen Jesus. "Jesus in our time, a new nail. Hallelujah!" sounded the refrain of the orthopaedic gospel choir.
As with many new inventions, however, it had its teething problems. It once happened that it accidentally self-ignited and sent the patient to the moon travelling faster than the rocket Saturn 5. When the patient returned to earth, with Glenn Miller's Moonlight Serenade still ringing in his ears, he was upset and he made a formal complaint to the director of the hospital. The director agreed with the patient and he said it was a justified complaint. On behalf of the hospital he delivered a sincere apology to the patient and he thought "What are they up to? Sending patients to the moon? They could at least have tuned in Beethoven's Moonlight Sonata for such a long journey."
In the aftermath of this lecture on his newly invented nail he was invited to the World Exhibition of Adult People in Paris 2009. At the exhibition there was an assortment of adult people demonstrating their skills. The motto of that year's exhibition was "Adult people are sensible and understand things" and the exhibition was much visited by children and teenagers who appreciated when Napoleon, with his Napoleon hat on his head, together with the other participants paraded under the Arc de Triomphe and down the Avenue des Champs-Élysées on the last day of the exhibition. When he came back from the exhibition he saw that there hung a fresh codfish on the outer wall of the hospital, obviously one of his colleagues had been full of enterprise. This was a routine they recently had adopted, to show the other staff of the hospital and the public that they had invented a new nail, something corresponding to the white smoke from the chimney of the Sistine Chapel when a new Pope had been elected in Rome. It was Napoleon who had come up with this idea, cardinal as he was. When the gulls had removed most of the codfish and only an empty skeleton remained they knew that it was time to invent another nail. Napoleon liked codfish. When he had difficulties in falling asleep at night he used to put a codfish under the pillow and it worked. He even recommended his patients to put a codfish under the pillow if they could not sleep at night. If it did not work he told them to put two codfish under the pillow.
There was a rumour going on that a crackpot in the middle of nowhere had written a feasibility study on the possibility to eliminate the deformity of the hip joint after Perthes disease and that without any surgery performed. It was evident to everybody that anyone who had such ideas must have some mental issues and they were right. His long-time excessive interest in Perthes disease had made him a little funny in his head and eventually he got the crackpot syndrome. This syndrome consists of four delusions affecting his view on himself and a deranged perception of the world surrounding him. The first delusion affecting his view on himself was "I don't exist". This was explained by the fact that he had secluded himself from the outer world. He had to do that in order to get enough time to think about Perthes disease and to read so much literature as he could about relevant sciences he came across. Concerning Perthes disease he had the view that he at least understood something but that everybody else did not understand anything at all.
The second delusion was "I don't know anything". This delusion had evolved gradually while he was beginning to understand how much there was to read and understand when pursuing his own theory about how to treat the deformity after Perthes disease and how many unsolved problems there were. Finally he gave up and said "I don't know anything" and this view of his later got permanent.
The third delusion was "I don't know what I have been doing in my life". This was explained by the fact that his line of thinking concerning Perthes disease was determined by factors outside his own control. During his time in school gene therapy had not yet been established, he did not know anything about scintillators, synchrotrons and Monte Carlo methods. Growth factors in bone were poorly understood. Sciences as optogenetics, synthetic biology, synthetic morphogenesis and synthetic enzymes did not exist. During the years his line of thinking suddenly and without warning had to adapt to this scientific progress several times. "Now you have to take this new knowledge into consideration, you fool!" It was as if the outside world determined and played with his life and he himself was a passive integrator of newly arrived knowledge. The fourth delusion was "I am a crackpot". He understood that he was a crackpot so in this sense he had a good insight into his own mental derangement, he even could enumerate the four delusions.
In addition to these four delusions a patient with the crackpot syndrome has a disturbed perception determined by the topic of his long-time excessive interest. In his case, when he was confronted with an orthopaedic surgeon he did not see a human being as normal people did. Instead, he saw a six-metre long saltwater crocodile from East Timor weighing one ton and with an appetite for hip joints.
On the internet he had come across a photograph depicting patients with Perthes disease and standing among them an orthopaedic surgeon. He printed this photograph and ordered a painting that interpreted his own perception of it. In the foreground of the painting there were some children with Perthes disease and standing among them an orthopaedic surgeon with a high ranking according to the Eurovision Smiling Contest. In the background a six-metre long saltwater crocodile from East Timor weighing one ton dressed in a doctor's white coat and sitting at the dinner table beside a mountain of femoral heads which had been collected from prosthetic joint operations on former patients with Perthes disease. The crocodile was having a meal consisting of these femoral heads, which he regarded as a delicacy, crunchy and with a superb taste, together with potatoes au gratin, sauce, vegetables and a glass of red wine of a good vintage. The painting was given the name "Perthes disease in the young hip - does it necessarily do well?" (1) and was for a long time on public display at the National Gallery in London before it went on a tour to museums all over the world.
The painting also appeared as a mural painting in Palazzo di Mancanza di Giudizio in Florence where there once was held a conference on Perthes disease where adult people under the supervision of the Kaiser and true to their usual habits competed with each other to give the most boring lecture. Afterwards they did not know what to do but finally they agreed that after a ceremonial flourish of trumpets they would establish the recently acquired insight that one plus one equals two. When they had sobered up and they went home from the conference they felt spiritually elated.
Besides the mental issues everybody was convinced that the crackpot had and which had left their mark on his peculiar expositions his idea was also rejected on religious grounds because it was in opposition to the orthopaedic confession of faith which stressed the importance of loading as much as possible of metallic and plastic materials into the population. A normalization of the anatomy of the hip joint after Perthes disease would make a prosthetic joint replacement later in life unnecessary and this could impair the annual report of the Vatican Mining and Production Lim and that would not be looked upon graciously by the Vatican. For that reason, it was decided that the crackpot must be publicly punished by dragging him to the market square and placing him face down on the ward sister's lap where she repeatedly would hit him on his bottom with a carpet beater as a warning example to the public and to teach him manners which he obviously was lacking.
Dr. Peculiar worked part-time as an orthopaedic surgeon and part-time as the head of The Institute of Applied Madness. The task of the institute was to describe and analyse madness in its various forms and to propagate it throughout society both nationally and internationally. Dr. Peculiar appreciated and enjoyed madness. He was one of the most prominent connoisseurs of madness in the world. The Institute's greatest success had been during the second decade of the third millennium when they managed to have their favourite candidate elected President of the United States. That really was an extraordinary achievement and the staff of the institute never had had so much fun as during those four years. Such an exposé of madness rarely had been seen at such a high political level before. That it was the Institute that arranged for all that has been a well-kept secret. Dr. Peculiar's standpoint was that the development of orthopedic surgery must be driven by ideas which at first sight seemed mad and the persons to whom the ideas were presented were unpleasently affected or began to laugh. The madder an idea seemed the better it was. He regarded Napoleon and the Crackpot as two admirable prominent figures, as orthopedic surgeons of the future.
To treat his own sleeping problem Dr. Peculiar had a flowerpot fastened on the top of his head with a strap under his chin. Dahlias and tulips were his favourites in this regard. Dahlias for uninterrupted sleep, tulips for uninterrupted sleep with pleasant dreams and on Saturday nights tulips with 10 ml of Cointreau liqueur in the planting soil for uninterrupted sleep with very pleasant dreams. He was a man of many tulips. Sometimes he had discussions with them, they helped him to shed some light on various kinds of madness in the world. He was immensely popular with the tulips, they were grateful for the Cointreau liqueur, it vitalized their sex life so there were many tulips in the garden. His unusual behaviour could be witnessed by everyone when he was lying on the lawn and talking to a tulip. On Saturdays he put up a booth with tulips in the market square and a sign with the text "Understand the world better - buy a tulip". Now and then he forgot to remove the flowerpot from his head before he came to work. It looked a bit strange when he was calling patients up in the waiting-room and he still had the flowerpot on his head. Sometimes Dr. Peculiar's patients disappeared. The relation between doctor and patient could at times topple over, not only when Dr. Peculiar had dressed up as count Dracula and switched on the tape-recorder with ghostly music but at other times to. Then Dr. Peculiar hit the patient's head with a hammer and bricked in the patient into a wall in the cellar. Dr. Peculiar's favourite author was Edgar Allan Poe.
Dr. Peculiar is famous for having invented the "egg-test" which is used to identify an orthopaedic surgeon among other physicians. The theoretical background is that an egg is intimately connected to the philosophical question: What came first, the hen or the egg? In the context of LCPD this question is like the question: What comes first, the fracture or the ischemia? Because this question is very embarrassing for an orthopaedic surgeon, the sight of an egg will cause a similar reaction in him as when count Dracula sees a crucifix. The test is performed by the examiner displaying an egg in front of a group of physicians and the physician who immediately looks terrified, shies away, and raises his arms to protect himself from the egg is the orthopaedic surgeon. An orthopaedic surgeon never has an egg for breakfast. Whatever you do, do not serve an orthopaedic surgeon bacon and eggs. He might smash the frying pan on your head and that could be dangerous. If you see an orthopaedic surgeon attacking people in town with a frying pan you know he has been served bacon and eggs.
The orthopaedic surgeon's inability to understand the aetiology of LCPD, his inability to avoid the deformity of the hip joint predisposing to arthrosis leaving the patients handicapped already in their early twenties, in some cases, and his disillusionment and talk about prosthetic joints all the time, affected him, he became a bore. In fact, he was an honorary member of The International Society of Crushing Bores and that for a reason. He was so boring that his wife had to shave him in the mornings because if he saw himself in a mirror he fell asleep. When on a Saturday afternoon he went to the ZOO together with his companions and he accidentally fell over the fence down to the lions, the lions did not bother to attack him because they thought he was too boring. He was so incredibly boring that the local bus company had forbidden him to use their services because once when he had embarked on one of their buses all the other passengers fell asleep. Even the bus gave up, so the driver had to park it beside the road before he too fell asleep. Dr. Peculiar was aware that his colleague was such a bore and he feared that one day his boredom would be transformed to a black hole of boredom which would engulf the earth and that would be the end of it.
One day when he arrived at work the orthopaedic surgeon with the incomplete ability related to LCPD was in an awfully bad mood. He had the day before received information from the system of taxation concerning lots of back tax to pay. In the morning, his car would not start so he was half an hour late. On his way to the hospital, he was stopped by the police because of speeding offence. When he arrived at the hospital, he was in such a bad mood that he had to take it out on somebody. He could not take it out on the ward sister because then he knew he would get beaten up in a way he would never forget but he could take it out on medical students. He decided to kill one hundred medical students by forcing them to attend his excruciatingly boring lecture on LCPD. The only thing that could soothe him and calm him down was the death of these one hundred medical students caused by such a lecture and he actually managed to do it. He actually managed to kill one hundred medical students who were attending his excruciatingly boring lecture on LCPD. What he did was that during the first two hours of the lecture he burst out in a cataclysmal eruption about the inability to define the cause of the disease. By now he had lost his head completely and during the following two hours he repeatedly and hysterically shouted at the students that once the deformity of the hip joint had appeared it was nothing to do about it, until he exhausted fell down on the floor and stared at the ceiling as if he wondered if Providence would have mercy on him and relieve him of his suffering. When he had managed to get up on his feet again, he devoted the last two hours of the lecture to an irrelevant and protracted wordy gibberish about butter, flour, black pepper, onions, potatoes, tomatoes, and chicken, but that was a mistake. It was a list that his wife had given him regarding purchases he was going to make in the supermarket on his way home. After the lecture, he was admitted to the psychiatric ward, and his prospects of ever being discharged were considered as poor. "Death by boredom" was the medical examiner's verdict after examination of the deceased one hundred medical students. The director of the hospital was quite upset because of the orthopedic surgeon's brutal lecture and that was understandable. After all, when chicken is on the menu, a much better alternative than potatoes would be rice and curry sauce. "What's the matter with him? Is he totally daft when it comes to cooking?"
The Crackpot's condition had deteriorated, and he too had been referred to the psychiatric ward. He did not respond to speech, and he only lay in his hospital bed persevering: "I don't exist..., I don't know anything..., I don't know what I have been doing in my life..., I have the crackpot syndrome..., I don't exist..." An NMR was performed which showed that his brain had shrunken to the size of a walnut which without aim and purpose was swimming about in a liquid-filled container. It was happily waving at the observer because it had always enjoyed getting some attention. It was feared that the Crackpot had contracted the malignant variety of the crackpot syndrome in which the brain continues to shrink until it finally disappears completely and the patient dies. There had been an epidemic of this frightful disease during the 60's when orthopaedic surgeons tried to figure out the aetiology of LCPD. It was concluded that they had been caught in the eternal question "Which comes first, the fracture or the ischemia?", a question they could not answer, and which finally drove them mad. They all began as young and promising and ended up as acerebral figures until they finally died without having understood anything whatsoever. There were so many of them that it was decided to bury them in a mass grave. They were piled up on the churchyard in waiting for the mass grave to be ready. Finally, the caterpillar came and shovelled them into it. Dr. Peculiar had a painting of this scene in his office which he called Portrait of Madness or Young and Promising. Dr. Peculiar also had another painting with a similar motif. Fifty orthopaedic surgeons participate in a conference on LCPD. The conference takes place at a churchyard. A mass grave suitable for fifty people has been dug. The Reaper is sitting at a table nearby. A caterpillar is also present, the driver has just drunk his coffee and had had a sandwich and now he is waiting. He is just waiting. Dr. Peculiar called the painting Scepticism.
It was time for Napoleon's nail to be baptized. All over the world the church bells rang for three days. "Our prayers have been heard; a new nail is born." It was a proud day for Napoleon when the priest gave the nail the name Almighty. Congratulations arrived from both the Pope and the Kaiser. A specimen of the nail was placed in the vitrine where the cultural heritage of the clinic was kept. The most prominent nails in the vitrine now were Almighty, Splendour of God, Midnight Blues and A Cup of Tea in the Desert. ("Nurse, pass me a Splendour of God please ..."). Three more nails and the kingdom of heaven would be just round the corner.
A specimen of Almighty also was sent to The Chapel of The Holy Nail in London. The chapel had been built on the initiative of the Pope. It was a cosy chapel with religiously inspired works of art on and at the walls and a minor library and a cafeteria nearby. The art collection included a portrait of the patron saint of the orthopaedic nail and portraits of orthopaedic surgeons who had been canonized because of distinguished inventions of orthopaedic nails from the Iron Age to present times, among them Dr. Ping Pong, Dr. Wilhelm von Vielhammerung, Dr. Herbert Pferd, and Dr. Totemo Kugitachi. During the Shu dynasty in China, Dr. Ping Pong manufactured the first orthopaedic nail made out of iron. He also invented table tennis and his descendants have made the China of today a prominent nation in this sport. During the Thirty Year's War, Dr. Wilhelm von Vielhammerung invented the "Trinail" with which it was possible to join three pieces of bone instead of only two pieces of bone. Dr. Pferd manufactured the first orthopedic nail equipped with a pony-tail. He was good at athletics, especially running but also high jump and long jump. Dr. Kugitachi was a Japanese orthopedic surgeon in the thirteenth century. When the Mongolians under the leadership of Kublai Khan, grandson of Djingis Kahn, tried to invade Japan in 1274, Dr. Kugitachi made a significant contribution to the defence of Japan by throwing orthopedic nails at the Mongolian intruders. In this he was so successful that Japan's ministry of defence decided to develop his orthopedic nails to a submarine based, long-range, high-precision targeting, hypersonic missile system, so-called "Kugitachi-missiles". If you have had a Kugitachi-missile hitting your house or your garden, you can lodge a complaint against the nearest orthopedic clinic. They usually have a special desk for that, "Complaints regarding Kugitachi-missiles. Please take a queue ticket". In fact, there had been a few occasions during weekends when the Crackpot had relaxed at home in his garden, and suddenly, a Kugitachi-missile had bored itself down into the lawn only a few feet away from him. He knew that there were those at the clinic who did not approve of his ideas and that they had taken the matter into their own hands to put him to silence.
In earlier times, orthopedic surgeons who had invented a particularly prominent nail could, apart from canonization, be granted an ascension. It was a spectacular sight where the trajectory to heaven was marked with light. If there were several orthopedic surgeons who awaited ascension the ascensions were performed at the same time and the lights which marked the trajectories could have different colours so that it looked like fireworks on New Year's Eve. In modern times the ascensions were replaced by canonizations because of fear of collisions with aeroplanes. The last ascension was performed in 1923 and was granted the French orthopedic surgeon Alois Nigaud who had manufactured an orthopedic nail with a built-in music box which played the Marseillaise in repeat mode. Unfortunately, he had forgotten to implement a function which switched the music box off so everywhere the patient went people stopped what they were doing and began to sing the French national anthem. The painting "The Ascension of Dr. Alois Nigaud" decorated the walls of the chapel.
The chapel was often visited by orthopaedic surgeons who sought inspiration for the invention of the next nail. It was an emotional moment when they during the service accompanied by beautiful and impressive organ music sang hymn no. 72, "Anthem to The Holy Nail", and hymn no. 145, "Holy Nail, in Thee We Rejoice".
In the meantime, the crocodile from East Timor had caused a scandal. On a stressful day when he had worked in the emergency ward there were so many patients that he had not had time for lunch. After work he wandered about in the corridors in search for something eatable until he finally found an appetizing colleague in his office. He attacked him ferociously and ate him. Afterwards he spit out the indigestible parts as the clothes, wallet and glasses and ended the session with a loud "buuuuuuurp!" The other doctors made a formal complaint to the director of the hospital and said it was a problem of the working environment. You could not have a crocodile wandering about in the corridors eating the staff.
Napoleon had made progress in his work with robots. To replace the colleague who recently had been eaten by the crocodile he had 3-D printed a new orthopaedic surgeon. It was the first 3-D printed orthopaedic surgeon ever. The Crackpot, who recently had recovered to his habitual state, once met him. He had written on the robot's screen: "Perthes disease. What to do?" The robot answered: "You should find the cause of the disease". The crackpot typed: "Noninvasive envelope engineering. What do you think about that?" This question caused the robot to stammer, his right eye rotated counter clockwise, his left eye rotated clockwise, smoke came out of his ears and on the screen it read: "Critical malfunction. On your behalf, please consult a psychiatrist. On my behalf, please consult technical department for an update of my software".
The reason for the Crackpot's improved mental state was that he had got rid of the eternal and lethal question "Which comes first, the fracture or the ischemia?" by stating that it was impossible to answer that question because it was impossible to perform an ACPS-measurement. Instead, he turned to the problem of NEE with synthetic enzymes and synthetic morphogenesis and that prevented the continued shrinkage of his brain and his own death, even if he knew that he was not going to see any progress in that field during the remainder of his life.
It is a sunny summer afternoon in the garden. The birds are singing, and the sky is clear. Dr. Peculiar is lying on the lawn and discussing world events with a tulip. Orthopaedic surgeons are sitting on tree branches high above the ground as birds but they are not singing. They have climbed the trees to be closer to God and to receive divine inspiration for the invention of the next nail. Napoleon, the Crackpot, and the Crocodile are sitting at a table on the lawn and are having a chat with each other. Napoleon and the Crackpot are having a cup of tea and some cookies. The Crocodile is having a cup of tea and some femoral heads. The painting is called "Afternoon Tea at the Hospital".
When the Crackpot had presented his feasibility study on NEE it was time for him to act. His goal was to bury LCPD as a viable topic for research. The overall goal as regards LCPD was the normal anatomy of the hip joint and he thought that the only procedure which could achieve this goal was a practicable NEE. The cause of the disease would never be found because an ACPS-measurement would never be possible. A treatment of the disease (weight-relief, containment) could not in the majority of cases prevent a deformation of the hip joint because a treatment would never be able to bring back dead bone cells to life. If you wanted to bring back dead bone cells to life you would have to move back in time and eliminate the cause of the ischemia and for that you would have to know the aetiology of the disease and you cannot know the aetiology because you cannot perform an ACPS-measurement shortly before and during the beginning of the disease. It is as simple as that. If the patient already has a deformation of the hip joint at the time of diagnosis it is even more obvious that a treatment cannot prevent it, it already exists. The only procedure which would be able to prevent a life-long deformation of the hip joint caused by LCPD was a feasible NEE. Because NEE in the foreseeable future would be impossible to perform the only reasonable measure was to bury LCPD as a topic for research with the exception of research aiming at making NEE feasible.
There were others before the Crackpot who also regarded LCPD to be a totally hopeless problem which never would find a solution and who also wanted to bury it as a topic for research because research focused on the aetiology and the treatment would never lead to anything and was a waste of resources. The Pope, however, had always rejected a funeral because something was missing. That which was missing was the Trinity of LCPD: the aetiology, the treatment of the disease process and the third and missing part, the treatment of the whole deformation in itself when the disease process had ceased. In order for a funeral to be granted a feasibility study on the post-disease treatment of the whole deformation of the affected hip joint had to be written. As no one had written such a feasibility study the Crackpot in a most glorious way did it. It was not necessary that the feasibility study outlined a treatment which likely would be possible in the near future, it should only give a broad outline to the first attempt to such a treatment which the present status of science allowed and a hint to the difficulties linked to such a hypothetical treatment regardless of the magnitude of the problems associated with it. The purpose of such a feasibility study was to explain the meaning of the Trinity of LCPD and to open a domain for speculation. The Crackpot thought that a funeral would simplify matters. You could rack your brain forever trying to find out what the aetiology was without understanding anything but that would be unnecessary after a funeral. Then you just had to hammer in the nails of today and to be perfectly happy. Now when he had written the feasibility study the Crackpot applied to the Pope for the funeral of LCPD. As an enclosure he attached his composition. After a couple of weeks, the decision by the Pope arrived. The Crackpot got what he wanted.
The funeral service took place in San Pietro in Vincoli in Rome and began with Pachelbel's Canon and ended with Air by Johann Sebastian Bach. The funeral cortège proceeded to the tones of Frédéric Chopin's Marche Funèbre and Tomaso Albinoni's Adagio to the burial ground. The chief mourner was Coxitis Simplex who was dressed in black and she was crying. The partial death of LCPD had been a severe loss for her. There were those who said that she had had an affair with LCPD. Septic Arthritis was also invited but he had been knocked down by a drink-driver in a Penicillin so he could not attend. The Crackpot looked content. Everything went according to plan and his mission had been accomplished. Napoleon did not have a special interest in LCPD and he looked rather indifferent. His interest was to replace the human being with a robot as a solution to the problem of diseases. He was accompanied by new varieties of 3D-printed orthopaedic surgeons because of the uncontrollable appetite of the crocodile from East Timor, who had arrived just in time for the funeral after a visit to the dentist. Two non-robotic orthopaedic surgeons were holding a newly invented nail between each other and were discussing its merits. Dr Peculiar was engaged in a conversation with a bouquet of tulips concerning the possible resurrection of LCPD as a suitable area for research. The tulips said that a resurrection only could be decided by the Pope. The biggest wreath was marked with the hammer and sickle and was sent by Josef Stalin. The painting depicting this defining moment in orthopaedic surgery, "The Funeral of LCPD", was later to be world-famous.